Iron Maiden’s lineup as it has stood since 1999: Dave Murray (G), Adrian Smith (G), Janick Gers (G), Bruce Dickinson (V), Steve Harris (B), and Nicko McBrain (D).
Just six months after our Judas Priest concert, Omri and I found a chance to see Iron Maiden in Concord, Northern CA, on Tuesday evening, September 27, 2022. This was a date on Iron Maiden’s “Legacy of the Beast” world tour. I didn’t know this, but “Legacy of the Beast” was a successful video game that the band launched last decade. The tour was originally scheduled for 2019 and was then postponed for years due to COVID. While waiting out the pandemic, Iron Maiden recorded and released its 17th studio album, Senjutsu.
Taking our seats high stage left. Iron Maiden is still drawing new young fans along with lifetime diehards like me and the silver-haired couple behind us.
Iron Maiden has been one of my favorite bands since I fell in love with Piece of Mind in 1990. I’d seen them live at least twice before: The 1992 Fear of the Dark tour (before Omri was born!) and the 2005 Ozzfest (the San Bernardino performance with the now-infamous tiff between Bruce Dickinson and the Osbournes!).
It was a different concert experience this decade. I was impressed by numerous themes this time, not least of which was their longevity and stability. When I first saw Iron Maiden live, I never would have guessed that I’d be seeing the same five guys (reunited with Adrian Smith) 30 years later! Despite that, the band is still living in the present and reinventing itself. And the stage spectacle of an Iron Maiden concert has gotten absolutely colossal.
The highwater mark of Iron Maiden’s career was the first trilogy of albums with Bruce Dickinson: Number of the Beast (1982), Piece of Mind (’83), and Powerslave (’84). When I saw them in decades past, they stuck to this canon for the most part. On this tour date, they were determined not to be a nostalgia act. They came out of the gate with three songs from their new album! I have now learned that these three tracks were Senjutsu, Stratego, and The Writing on the Wall. I think that this was a very gutsy move. I’m sure that most people in attendance had never heard these songs nor were particularly interested in hearing new material. By playing three new songs in a row, the band sent a message that they still take themselves seriously as a creative force, and they demanded us to give “new Maiden” a chance.
I believe it paid off. These songs were gripping and presented extremely well. The set opened with a drum set flashing like lightning, and then the band played in a blue-tinted Japanese village with a Samurai Eddie. The Writing on the Wall has an incredible animated video that would have fit perfectly into the Heavy Metal movie, with phantom motorcycle gangs and Eddie wreaking mayhem. This album’s plodding tempos and dark atmosphere remind me of TheChemical Wedding, a Bruce Dickinson solo album from 1998 that features Adrian Smith on guitar. I surmised (correctly, as it turns out) that Dickinson and Smith did a lot of the songwriting on this album. By the end of the third song, I was surprised by the concert’s direction but convinced that the band is still an important creative force.
Though I got some good photos from this concert, my video footage isn’t very impressive. I ran into some copyright notices while trying to post videos as well. I will link to pre-existing videos on YouTube.
Then they started to dip into their hit list. By the time the full set was over, about half of their selections were drawn from the three bestselling albums mentioned above. There were a few more post-1990 selections, including two songs from the ’90s when Bruce Dickinson and Adrian Smith had taken a hiatus! Sign of the Cross and The Clansman were originally sung by Blaze Bayley. These songs were new to my ear, and very unexpected choices, but I especially found Sign of the Cross to be a strong track.
Everything about the concert was HUGE! I don’t remember such theatric spectacle in decades past. Two giant Eddies came out to wield swords. The set changed from the Japanese village to a gothic cathedral for Revelation, and then we got a fiery hellscape for songs like Sign of the Cross and Number of the Beast. When they played their eponymous song, the inflatable Eddie-monster head behind them was the size of a hot air balloon craft. For their final encore, Aces High, a half-size WWII fighter jet was suspended over the stage. Bruce Dickinson made a few wardrobe changes to suit the songs. I didn’t remember earlier Iron Maiden concerts being so extravagant with their elaborate sets, enormous props, and pyrotechnics. I think that they have been continuously developing their stagecraft year after year, to the point that their live shows are now in the same league as Kiss, Pink Floyd, and The Rolling Stones.
Senjutsu-Eddie towers over Dave MurrayA whale-sized Eddie head“Aces High” fighter jet
The musicians are all still performing at their peak. Dickinson can’t quite reach all the glory notes that he hit in his youth, which is understandable after a bout with throat cancer. But his voice is still as strong as ever in his freakish G-to-high-C tessitura.
The only thing that an Iron Maiden fan can “complain” about is that their repertoire is now far too lengthy for one concert. I would have liked to hear Dance of Death, Phantom of the Opera, Mother Russia, the list goes on. They are not currently performing any songs from Somewhere in Time or Seventh Son of a Seventh Son, their first two synth-heavy albums. I have long wondered why Harris chooses to keep three guitarists in the band instead of swapping one of them out for a keyboardist.
Interestingly, as I write this, I see that their next planned tour, the Future Past Tour of 2023 – ’24, will “revisit Somewhere In Time“, which is probably my favorite Iron Maiden album of them all. Maybe I’ll see you there next year!
I hadn’t been to a rock concert in years. (Has it been decades now?) They’ve gotten so damned expensive, and I’ve already seen most of the greats at least once. You know, last century. Now I have a younger girlfriend, Omri, who is discovering rock music for the first time. When she got hooked on some Judas Priest videos, and then discovered that they were on tour near us, I couldn’t resist. We attended the “50 Heavy Metal Years” tour in Phoenix, AZ on March 16. We loved it! It was one of my favorite concert events ever. But here’s my full critical take.
Omri and I take our seats
Queensryche was the opening act. This was another of my favorites back in the day, so I made sure that we got to the concert in time for this full set. Queensryche and Judas Priest now both squarely qualify as “Dinosaur Rock” bands. Their commercial success, popularity, and influence peaked long ago. But that’s what I like about concerts like this. Their casual fans — the ones who’d fill stadiums when the bands were trendy — stayed at home. We got to see these powerhouse acts in a theater (the kind where you’d go to see a play or musical) with a core of passionate lifelong fans. Omri was surrounded by middle-aged men. They were excited to see her, not just because she’s beautiful, but because she’s a young new recruit! They couldn’t stop regaling her with tales of their concert history and recommending bands to listen to.
For my sensibilities, the sound crew hasn’t adapted to the small-venue phase of these bands’ career. It was far louder than necessary for a space that size. I know, who ever complains about sound levels at a heavy metal concert?! But honestly, sometimes less is more. Stadium speakers weren’t meant for theater acoustics, so the sound was a bit mushy for my liking.
The fundamental question that Dinosaur Rock fans must ask ourselves is whether to accept changes in personnel. There are many purists who lose interest after one original member rotates out. While I have my favorite lineups, it’s getting late in the game for rock history. Changes are inevitable. I have come to appreciate the bands that persevere for decades no matter what they have to do to survive. If we can accept turnover in our favorite sports teams, why not bands?
Queensryche, featuring two original members and three newer ones.
That is a particularly salient question for Queensryche, which has been without signature-sound vocalist Geoff Tate for several years now. The two remaining original members are guitarist Michael Wilton and bassist Eddie Jackson. The band opted for a Tate sound-alike singer. There aren’t many of them in the world, and I have to admit that they plugged in a pretty damned good replacement in Todd La Torre. I was especially impressed when I read later that La Torre considers himself primarily a drummer, and only started singing as an afterthought. I sometimes feel that La Torre goes out of his way to mimic Tate down to every last inflection. He gets into that Uncanny Valley where he sounds so close to Tate that it bothers you that it isn’t Tate. I’ve seen an interview where he claims to have found his own distinct style. I don’t hear it, but again — he is definitely up to the challenge of the Queensryche repertoire.
I was surprised that Queensryche kept digging into its earliest albums. Although the band has albums as recent as 2019, every single song in this set came from 1983 – 1990. I was doubly surprised when Judas Priest did the same thing. The only song that postdated 1990 in this entire concert was Judas Priest’s “Lightning Strike” from 2018. Of course, the old material is what most fans came to hear, but bands usually like to try circulating and selling their newer material. That especially would have made sense with the “50 Heavy Metal Years” theme. Having heard a few 21st century Judas Priest songs, frankly, I think they would have been solid contributions to this set. Nevertheless, I have to agree, I am not very familiar with either band’s repertoire since 1990, so I was pleased to hear many old favorites. Queensryche, in particular, played so much of its old hardcore geek metal that it almost seemed like a deliberate attempt to weed out casual Empire fans!
A few other choices surprised me. Judas Priest played some tracks from my favorite under-rated albums, such as “Desert Plains” (Point of Entry, 1981) and even “Blood Red Skies” (Ram It Down, 1988). I don’t think I’d ever heard Judas Priest play a song from Ram It Down live; for years they seemed to go into denial that they’d ever made this album, the long-lost sleeper between Screaming for Vengeance and Painkiller. Judging from reactions around me, Blood Red Skies was actually a fan favorite for the evening (Omri agreed!)
I created a YouTube playlist of both bands’ full set lists for this evening’s show. These are official videos, many of them quite old, not recordings from the concert.
This playlist presents all the songs played at this concert, in order.
And now I must come to my most controversial assessment. Rob Halford’s voice is aging. I heard him in concert at least three times in the ’90s and ’00s. Each time, I was blown away by the strength, elasticity, and purity of his voice. I give him kudos to what he is still doing now, but I could tell that he is simply not capable of keeping up with his younger self. As a former heavy metal vocalist wannabe myself, I know the pains of navigating the break between chest voice and head voice. Most mere mortals like me have a gap there spanning about a third, where both vocal modes are weak and crossing that point is vocally exhausting. Halford used to breeze through that part of the range like a canary. Now he falls into a mute spot there. His upper range is no longer clear. Apparently, the only way he can reach his highest notes now is with Bryan Johnson-esque fry vocals. I don’t see or hear many people discussing this. Maybe it’s just me, or maybe people don’t want to say anything because we all love Halford.
For me it was kind of emotional, though. I have a 30-year history with Judas Priest concerts. Now I feel that an era has passed. The Rob Halford that I knew just isn’t there anymore. Juxtaposed with the Queensryche performance, it made me ponder an unthinkable question. Would I prefer to see Judas Priest with Ripper Owens? I’d choose 20th century Halford over Owens any time. (That’s what recordings are for). But honestly, I think that Owens (who is two decades younger) is stronger than Halford today.
Speaking of the old-timers, it was great to see two other original band members there. Bassist Ian Hill has been in Judas Priest slightly longer than Rob Halford. The original dual guitar lineup of K.K. Downing and Glenn Tipton has now been replaced by younger blood. Downing’s replacement, Richie Faulkner, is phenomenal. He electrified the stage from start to finish. Tipton’s touring stand-in, Andy Sneap, didn’t make as much of an impression on me. He is better known as a producer, and he is not well embedded with this band yet. Tipton, who has Parkinson’s Disease, still plays in the studio. In fact, he still does a little touring too. He hides out backstage through most of the set, but then Rob Halford calls Tipton on stage to join the band for a couple of encore songs. Tipton coming in for “Metal Gods” got one of the biggest cheers of the night.
Tipton (L) and Hill
I am also happy to see that Travis Scott has been with the band this long. One of the interesting quirks about Judas Priest is that, through its entire heyday, it didn’t have a steady drummer. Travis Scott is “the new guy” who came on board for the Painkiller album. Now he introduces the song Painkiller every night of this tour, three decades later.
I’m old enough to have grown up while heavy metal music was being invented, and young enough to have not outgrown it yet. I was in the generation most shaped by this genre, which I’m sure seems intimidating to most Baby Boomers and kitschy to most Millennials.
This week, we middle-aged metalheads were shocked by the unexpected death of Mike Howe, lead singer of Metal Church. He was barely older than I. Metal Church was a thrash metal band — one of the earliest, purest, and best in that sub-genre — yet somehow they never became a household name. I first discovered their 1989 album “Blessing in Disguise” when a college friend lent it to me on cassette. Everything about the band impressed me. There were no weak links.
One thing you’ll notice about the band photo is that there were five members. This means that Howe was a designated vocalist. Unlike the quartets Metallica, Slayer, or Megadeth, whose singers were all primarily instrumentalists, Metal Church hired Howe only for his voice and front man stage presence.
Thrash metal is not about beautiful voices, though Howe could evoke a haunting tone in his midrange. He sang in what I call the “brat” style, that gritty falsetto that you hear in Led Zeppelin, AC/DC, Guns ‘n’ Roses, etc. It’s a sound that I couldn’t emulate even if I tried. I feel that “powerful” is the most apt adjective for Howe’s vocal performances. Also unlike many other thrash bands, Metal Church wrote rangy melodic vocal lines in the “power metal” style. Howe handled the melodies with spot-on pitch control and an intense up-front focus that is unusual for this style. I often felt that he adopted the growl of Megadeth’s Dave Mustaine and actually, well, sang with it. Howe recorded harmony vocals. Sometimes he doubled himself in octaves, which gave his voice a fuller sound. At other times, it was true harmony, which added great depth to the song. Metal Church’s music was always dark and virtuosic. Their lyrics were sometimes juvenile but usually thought-provoking.
If Metal Church is new to you, or if you “just don’t get” thrash metal, give this song a try first: the radio / video-friendly version of “Badlands” (all my recommendations appear at the bottom of this post). The vocals come in after just 12 seconds, and I think you’ll have to agree that, by the 1:00 mark, they definitely grip your attention!
If you’re looking to travel further down the Metal Church rabbit hole, I would next refer you to some of their great epic songs. “Anthem to the Estranged” is about people going through the worst moments of their life like homelessness or alcoholism. “Rest in Pieces” is about the sinking of the Titanic. “Little Boy” is about the atomic bomb dropped on Hiroshima. I embed my favorite versions of each video below.
As for their full albums, in my opinion “Blessing in Disguise” (1989) and “Hanging in the Balance” (1993) are in a class of their own. “The Human Factor” (1991) was from the same era, though that one escaped my attention until recently. After decades apart, Howe and Metal Church reunited for the albums “XI” (2016) and “Damned if you Do” (2018). I am not familiar with them at all. There are several other Metal Church albums with different vocalists.
And without further adieu, here are those recommendations:
Congratulations! The IMF has selected you to manage a grant of $8 billion to make the world a better place. You have great discretion over the budget. You may save some or all of this fortune away for your own financial security. You may consume to your heart’s content and let the money trickle down. You may invest in your favorite corporations or start a new one. You can form a charity.
Or …
You may choose to give most of the money to other people. Remember, your mission is to make the world a better place. Your gift portion must satisfy these simple rules:
You can divvy the money among any number N of people, from N = 1 (just yourself) to N = 8 billion (Every person in the world).
You must distribute the money equally among these N people. Nobody else will receive a direct payment.
Each person who receives a share will have full budgeting authority for that share. You can’t tell them how to spend it. However, they may not “regift” it. Only you have authority over slicing the pie.
Here are some sample scenarios:
N = 1. You keep full control over the whole $8B jackpot. Other people will complain, but you trust no one more than yourself to spend this money wisely. Just imagine the impact that your charities will have! Or maybe you can form a corporation putting thousands of people to work in productive and rewarding careers!
N = 8. You and seven friends will each control $1B. Is it worth watering down your share to diversify among a few friends?
N = 8,000. Now you must give your money away to people you don’t know. You will make these people all millionaires. Maybe they can invest wisely to make their communities better places.
N = 100,000. Each person in your pool will receive $80,000, enough to enjoy a comfortable living for a year. This could transform the lives of 100,000 families living in poverty. But … is this an unfair “handout”? Will they spend it wisely?
N = 200,000. Each person in your pool will receive $40,000. This could reach even more families, but with diminished impact.
N = 8 billion. Every person in the world gets $1. Although the fortune is now split with perfect equity, it has lost all power to do anything useful. It is also going to rich families as well as poor.
What value of N would you choose?
Everyone seems to have an opinion about the distribution of income and wealth. While it’s easy to say, “That’s wrong,” it’s much harder to follow up with, “And I’ll tell you what’s right.” I created this exercise to force you to state your position and then struggle with its imperfections.
The moral of the story is that wealth must go through two stages to do any good:
At some points in the economy, wealth must be concentrated. That’s the only way to build enterprises that do good works. (Are you listening on the left?)
Wealth must eventually flow from highly concentrated centers to less concentrated ones. That’s the only way to keep the economy alive. (Are you listening on the right?)
This exercise also addresses such questions as, “Who gets the wealth?”, “Who should decide?”, and “What strings should be attached?”
Please share your thoughts. I might follow up with another post describing how people think wealth should be distributed, how they think it is distributed, and how it actually is distributed.
A full solution requires many pieces: health, economy, politics, and teamwork. Click here for attribution1
I am researching and writing this primer to take a big-picture look at the COVID-19 epidemic. I announced it on Facebook in June and invited questions from my friends. What I originally envisioned as a single essay has now developed into an ongoing series of indefinite duration! Now that I have examined the pandemic from biological, medical, epidemiological, and social perspectives, today I consider the upshot: “So … what should we do now?!” How shall we resolve the three-way tug of war involving public health, the economy, and political peace? How should we conduct our lives until the virus is under control?
President Trump tweeted, “We cannot let the cure be worse than the problem itself.”2
Most people would agree with President Trump’s rationale. The keyword in this sentiment is “worse”, which is frustratingly hard to define. It depends on the costs and benefits of action vs. inaction.
Let’s suppose at its simplest level that cost is measured strictly in terms of human lives lost. One research team estimates that strict public health measures could save about a million American lives this year while causing around 100,000 poverty-related deaths. That is a nightmarish ethical dilemma. On balance, though, playing it safe with public health measures like stay-at-home orders would be justified. 3 The problem is that prevented deaths are invisible. Virtually nobody would celebrate the million lives saved, while the actual recession-related deaths would make headlines daily.
I got curious to look up the countries that had done best at protecting their economies, those that had done best to minimize infections, and those that had struck the best balance. The results surprised me. In the long run, there is no tradeoff. The countries that have done best at keeping their COVID-19 deaths down are actually those with the most successful economies now. 4 Although “lockdown” is a difficult short-term process, it allows for an earlier return to normalcy and therefore greater long-term recovery.
If numbers were the only consideration, the solution would seem “obvious”. With a truly rigorous, highly-enforced social lockdown for 2 – 4 weeks, we could put this pandemic behind us. That scenario alarmed us in March, but by now another 2 – 4 weeks would not feel shocking.
There’s another factor, though: political will. I’d be willing to horde groceries and stay home for a couple more weeks. I know that many of you would too, even some conservatives in small states. But we also know how ferocious the resistance would be. People would refuse to comply; the stricter the order, the harder it would be to enforce. The short-term pain would be undeniable. Some people would feel so angry and oppressed that they would develop permanent vendettas or even go Rambo on us. The emotional costs of such drastic action would simply be too high. Unfortunately, the longer this goes on, the more time the pandemic has to grow exponentially.
If the short-term and long-term solutions are at odds with each other, how else can we find the right balance?
II. Suggestions from the Left and Right
I seem to see two competing visions emerging.
A. The “Experts'” or “Liberal” Solution
Monitor hotspots
Locally tailor protocols, including face mask mandates, business closures, and prohibitions of mass gatherings, where and when appropriate
Increase the number and speed of tests where needed
Improve contact tracing and quarantine procedures
Wait for a vaccine
A good example of this model is California’s stay-at-home order, which was one of the first statewide responses in the United States and which is regularly updated. California counties are ranked on a heat spectrum (yellow < orange < red < purple < blue) which is now defined by availability of ICU beds. Business activities and freedom of movement are more strictly restricted in hotter spots. The state also recently launched the CA Notify app. When someone who uses the app tests positive for SARS-CoV-2, she can alert the app. Users who spend extended periods of time in proximity to her will then get notifications on their phones.
B. The “People’s” or “Conservative” Solution
Preemptively quarantine the vulnerable
Let everyone else get back to life as usual
Face masks and social distancing up to personal conscience
Wait for herd immunity
The conservative model is expressed in the Great Barrington Declaration. The preamble to this declaration indicates that its proponents are more concerned about government orders than the virus. The plan calls itself “Focused Protection” because it would focus on protecting nursing home residents and other vulnerable patients, while keeping children in school because they are much less susceptible. Many experts do not find focused protection to be feasible; flu pandemics illustrate that is not possible to effectively identify or quarantine the vulnerable population. 5 In fact, the apparent mass appeal of the Great Barrington Declaration is that it is extremely simple. The declaration is short and abstract, more a set of goals than a plan of execution.
III. My Humble Suggestions
This primer has discussed benefits and drawbacks to various prongs of the liberal and conservative approaches. Business lockdowns cause their own pain, and mandates lead to political friction. A vaccine could be years away in some parts of the world. With indiscriminate reopenings, we might reach herd immunity before a vaccine is available, but that process would kill tens of millions of people and would overwhelm hospitals to the point of causing millions more non-COVID deaths.
Some compromise will be necessary and optimal. 6 Compromise requires looking at this pandemic as a political problem, not strictly a medical or economic one. The political controversy is the main factor that tends to be left out when people discuss solutions. No plan is acceptable if it leads to violence or permanent vendettas. And no single plan will be acceptable to everyone.
Here are some abstract political principles that guide my thoughts.
“I’ll explain my position and respect yours.”
In a democracy, we define what is “right” by the people’s choice, even when it’s based on false premises. That is frustrating, but it’s a price we pay.
The more controversial a decision is, the more locally it should be made.
Consider externalities
Externalities are a fancy way of saying costs or benefits that one person’s decisions have on society around him. Most economics classes teach that an economy is most efficient when people are charged for the messes they make or rewarded for the messes they clean up. I’m a little surprised that I haven’t heard this topic being discussed widely this year in response to the pandemic.
When I consider these principles in sum, I conclude that each person, family, business, and government should assume the right and the responsibility for its own decisions. Here are some applications that would follow from this existential approach.
The people’s primary freedom is the right to decide how to carry out their lives. Face masks, social gatherings, and business closures should mostly be individual decisions. In fact, this already is true in reality. It’s difficult to enforce mandates on individuals, so people already are acting according to their own judgment.
In order to guide people’s actions, governments have a responsibility to educate: to provide data, science, and recommendations with justifications. Most people will choose to do the right thing and respect sensible recommendations. For instance, governments everywhere have been consistent about their advice to wear face masks. Even without a mandate, 85% of Americans already report that they regularly wear face masks voluntarily, including 76% of Republicans. 7 For conservatives, it’s that last step of the requirement that gets the blood boiling. Thus, the benefits of requiring face masks probably does not greatly outweigh the political ill-will.
Aristotle described three forms of persuasion: logos, pathos, and ethos. As someone trained in the sciences, I respond to logos: facts and logic. However, I recognize that most people base their values primarily on ethos (who is delivering the message) supported secondarily by pathos (emotions), then perhaps justified after the fact by heavily filtered evidence. In the United States, for instance, 1/3 to ½ of the nation is conservative. This constituency has decided that Anthony Fauci, Joe Biden, and all Democrats are bad guys. Many conservatives won’t listen to a word that Dr. Fauci or Governor Whitmer says, no matter how well it is supported by science. To reach conservative citizens, public health agencies must recruit conservative spokespeople. I can hardly think of a better example than Dolly Parton. This beloved red-state icon donated $1 million to the Moderna vaccine. In fact, federal agents have already suggested enlisting her as a spokesperson to encourage mask wearing in Knox County, TN. 8 What we need now is a concerted bipartisan campaign to encourage staying at home and avoiding gatherings as a patriotic call of duty, if not a legal command. Let’s start comparing the sacrifices that we ordinary citizens make to those of soldiers and policemen, part of a higher cause.
COVID-19 liability is a hot topic this year, and it should play an important part in our response. Ideally, people, and especially businesses, should be held liable for medical costs if they cause infections by high-risk behavior. Of course, the problem here is that it’s almost impossible to trace the origins of each transmission. A practical middle-ground would be a liability-reward system based on tolls, taxes, and subsidies. Maybe businesses can pay for population density permits on their property, with a discount if they require on-site rapid testing. Perhaps customers can pay a little extra by the minute or the mile to enter stores, ride buses, and the like. The proceeds from these tolls can fund medical treatment, vaccine and face mask giveaways, and rapid tests.
If a government does force a business to close, it ought to compensate for lost profits. In fact, I believe that it’s reasonable to interpret the 5th Amendment to the US constitution as requiring such payback: “nor shall private property be taken for public use, without just compensation.” In this pandemic, closing a business to mitigate the spread of a virus is a “public use”, and forcing an establishment to close is “taking” the property for that use. This business would continue paying its employees and vendors with the government bailout. On the hook for the costs, the government would have incentive to become extremely judicious with its closures.
There are a few more COVID-specific principles to help us make common sense decisions.
A higher current level of infections justifies more restricted behavior.
Stricter regulations are only sustainable over smaller places or shorter times.
The more vulnerable the person, or the people he meets, the more care is warranted.
States treat counties differently depending on their rates of new cases, rates of positive tests, percentage of ICU capacity available, etc. I made a 1% rule of thumb for myself. When the pandemic started, I vowed to stay out of areas where more than 1% of the population is actively infected. Today, it so happens that my neighborhood, city, county, state, and even the entire US is more than 2% actively infected. I obviously can’t “stay out” of these regions, but these levels tell me that it’s time to “stay in” as much as possible. While I can commit to locking down at home for a couple of days, it’s unreasonable to expect self-quarantine for months on end. It’s completely unrealistic to expect the whole world to hunker down for a year. I do find it reasonable to stay home for Christmas this year. It’s a sacrifice I’m willing to make because it feels like the right thing to do.
I don’t understand the rationale behind curfews, and I’m not sure anyone has evidence that they do any good. In fact, I would propose that businesses in high-risk zones should stay open 24 hours. Then customers could spread themselves out throughout the day. Hell, we could even offer graveyard shift discounts.
IV. Conclusions
It would be possible to end this pandemic within a month, but only with a coordinated and strictly enforced worldwide shutdown. If the pandemic were strictly a medical issue, or even a medical / economic issue, this solution would be a slam dunk. But we all know it’s draconian and unrealistic. Some people would suffer great loss, some would resent the lockdown for the rest of their lives, and some don’t even believe that the virus is real. Different people are swayed by different emotions or evidence, and some pay no heed to evidence at all. But they are all part of the democratic decision-making machine.
There is room for individualized response. In fact, that may be the only way to keep political tensions under control. We must allow some latitude for people and businesses to make their own choices.
On the flipside, freedom bears responsibility. Charge an extra $1 for a movie ticket in Canada, or 25% for bus fare in New York, and then let people decide what they’re willing to pay for. Use the proceeds for COVID-related medical expenses and to support businesses that have closed their doors.
In this way, everyone would come around in their own time. Even vocal conservatives will take care when they begin to feel more threatened by the virus than by human watchdogs.
COVID-19 is much more than a medical issue. The virus, and human response to the virus, have made 2020 feel like a time of war.1
What is guiding us — the fear of contagion or the contagion of fear?
About This Primer
I am researching and writing this series to take a big-picture look at COVID-19. I’m taking a step back from the daily news information overload and fact-checking the (even larger) load of misinformation. I announced this project in June and invited questions from my friends. It is now a series of indefinite duration. Part 1 covered the basics of viruses and coronaviruses. Part 2 dealt with SARS-CoV-2 on the level of individual health. Part 3 discussed the epidemiology.
In today’s installment, I take a turn from the biological to the social realm. The pandemic is much more than a medical issue. It has come to define the environment of 2020 in all aspects of our lives. Part 4 is “Coronavirus and Society.” I begin with the coronavirus recession. I then discuss the psychology and politics of how we think, feel, and communicate about this pandemic. What guides us – the fear of contagion or the contagion of fear? Why do different segments of society have such divergent outlooks on this event?
COVID-19 as a social and economic crisis is arguably more momentous than as a medical crisis. The only way to slow the contagion for now is to regulate travel and population density. As you well know, this keeps employees from work, it slows down consumer spending, and it shutters factories – in short, it is an economic wrecking ball. While the virus itself has harmed about 1% of 1% of us, our response to it has impacted us all.
A recession is defined as a period of at least two consecutive quarters of economic contraction. By that standard, the US and 18 other nations were already in recession by the 3rd quarter. 2 The forecast for the year is that the global economy will shrink by 4 – 5%, the deepest plunge since WWII. This is the first recession to slow down the growth of developing nations. Some economists predict that over 90% of all national economies will contract this year, a metric that makes this downturn even worse than the Great Depression. 3 The loss of jobs in the second quarter of 2020 alone was equivalent to almost 200 million full-time workers. 4
When economists describe this recession, a recurring theme is that demand and supply are both down. 5 This double-whammy impact is felt most strongly in travel and inessential establishments like bars and massage parlors. Not only are these businesses unable to provide their full range of services, but the customers have less discretionary money on hand. This will make recovery difficult, as there will not be an excess of demand waiting to meet recovering supply or vice versa.
Another significant effect is a transfer of economic activity from one sector to another. While restaurant dining is down, food delivery is up; TV on demand has taken over the movie theater industry. Online shopping has exploded. Many of today’s hot sectors (like nursing and webcasting) are hiring vigorously. However, it will take a while for employees to train and find jobs, and by then the short-term surge may have ended.
Some sectors are unequivocally depressed. Oil prices have tanked as people have driven less and airlines have slashed flights. This helps consumers but harms many of the poorest countries, which derive a large portion of their income from oil exports.
In some ways, the coronavirus recession is a tipping point for existing crises. There was already a major debt crisis in the 2010s. Now, government spending is breaking records. There have been numerous high-profile stimulus packages in the US and Europe. Small governments that are not accustomed to such bailouts are strained to the limits and are borrowing heavily. 6 Lockdowns are also exacerbating famines that were already alarming last year. 7
The two faces of the coronavirus – the disease and the depression – have us between a rock and a hard place. In the short term, we cannot ameliorate one without aggravating the other. Concerns about public health and the economy are all legitimate, and it seems politically impossible to find a balance satisfactory to everyone.
II. National And Partisan Differences In Attitude
An anonymous person on a forum asked, “Why do conservatives downplay the pandemic compared to liberals?“
The tension between public health and the economy is ages old, and political parties were already positioned on opposite sides of the divide. Conservatism might be described as an “economy first” philosophy. Conservatives resist spending money or changing behavior for new or uncertain threats. Liberal-minded thinkers are more receptive to accepting new problems and solutions, 8 and to paying for those solutions with government funds. These positions have been consistent at least since the 18th century, when economists sounded alarms about overpopulation. The same theme has played out with nutritional and medicinal advice, wildlife conservation, pollution, and climate change.
There is an important commonality to these modern liberal concerns. They are all “invisible” to the individual. When it comes to cosmic questions, conservatives feel more comfortable with traditional sources like religion. Otherwise, reality is conservatively defined by tangible direct personal experience. The conservative part of our mind is apt to think, “I burn gasoline in my car every day. My neighborhood is clean, and it snowed here last night. You can’t tell me that fossil fuels cause pollution or climate change!” It’s easy to conclude that warnings about fossil fuels are a fiction spun by someone with an agenda.
The liberal part of our mind may have an easier time seeing, believing, or caring about aggregate effects. However, liberal parties can take their concerns to extremes that are not clearly necessary. Public health threats are often detected in their early phases. We can’t really know the scope of the problem without predicting the future – and predictions often lead to worst-case-scenario anxiety. Furthermore, aggregate solutions do not always require rapid, radical changes for all persons.
The political divide is exaggerated by urban / rural differences. Viral contagion, like many other societal hazards, is most rampant in densely populated cities. Urban areas also happen to be more liberal in character than small towns and the countryside. Since ruralites don’t face the same infectious risk as urbanites, they often feel that city-made precautions do not apply to them. 9
B. Political Parties and Leaders
Most people are probably not conscious of why each attitude is associated with a different political party, but it doesn’t matter why. Once those associations are made, they become self-perpetuating. Well before the pandemic, the Republican and Democratic parties of the United States had already become hyper-partisan to the point of feeling contemptuous and prejudiced toward each other. Sociologists actually have a name for this state: affective polarization. 10 It has become more important to each party to defeat the other than to think in terms of a common interest.
Political leaders and the party rank-and-file reinforce each other. Politicians know and say what their constituents want to hear. Their behavior clarifies the party standard, which crystallizes quickly throughout the party. On the right, presidents such as Trump 11 and Bolsonaro 12 resist wearing masks, downplay the public health threat, and scoff at safety measures. Trump has said that wearing a mask “would send the wrong message” to his voters by making it seem like he is preoccupied with health instead of the economy. 13 In turn, 84% of Republicans trust the president more than they trust scientists. 14
Political parties can co-exist peacefully even when they have different values. They may self-segregate or irritate each other. The differences become more salient when one party imposes its values on the other, or even when one perceives an imposition. This year, generically speaking, conservatives feel that governments, corporations, and even judgmental neighbors are imposing “liberal” rules and restrictions upon them. Liberals feel violated when conservatives invade their space without safety precautions. In this quibble, the stakes are high.
C. National Differences
Some political leaders feel embarrassed about natural disasters getting out of their control, so they deny the problem or shift blame. The Chinese and US governments point the finger at each other, sometimes with completely unfounded accusations. 15 President Trump has alternately argued that his opponents are making a mountain out of a molehill 16 or, if it is a bad problem, it’s their fault. 17
The United States and western Europe, the homeland of the 18th century Enlightenment, are unique among the world in their esteem of individual liberty. 18 The rest of the world places higher value on being “protective of the collective” (to coin a phrase) even if it demands personal sacrifice. As I discussed in Part 3, Asians have a much easier time accepting government recommendations, and they wear face masks in the highest proportions.
Westerners, on the other extreme, feel threatened when the government tells them what to do, even if it is for the public good. This sentiment increases toward the right. Many conservatives deny that there is a public threat at all. The words that they associate most often with face mask mandates and social lockdowns are not even entirely economical; they include “freedom” and “rights”.
III. The Psychology of Uncertainty
Karen K. commented, “The speed at which guidance changes based on ‘emerging understanding’ of the virus is enough to make me trust no one.”
Mitzi M-H rhetorized, “How can we possibly know what it’s doing when the numbers are changing or inaccurate to start with?”
William B. rhetorized, “What’s going on with the WHO and the CDC? Why are there so many disparate studies and conflicting information?”
When it comes to the coronavirus, it’s important to remember a key issue:
There are many unknowns.
This butts heads with a universal law of human nature:
We hate unknowns.
As 21st century web addicts, we demand answers, and we demand them now! Unfortunately, clear answers are usually hard to find in the early stages of any sudden crisis. We ask, “How many infections are harmless and undetected? What causes more harm – the disease or the lockdowns? Will immunity last forever? When will vaccines be available?” We expect textbook right-and-wrong answers. Although many such questions are mathematically modeled, they usually have answers like, “We don’t know,” or “It depends.”
These are emotionally unsatisfying answers, especially coming from experts, and doubly so for people who are not accustomed to nuance. Unresolved anxiety then tempts us to conclude, “There is a simple answer, and someone knows, but they’re not telling me!” Then our imagination fills in the voids. We are highly prone to believing the next “satisfying” answer that comes along. 1This is the natural train of thought, especially for minds untrained in science and logic. Ironically, people who have such thoughts often believe that they are experiencing brilliant insights or revelations and feel uniquely enlightened. 19
It’s okay to accept that knowledge has boundaries, often blurry ones. That’s especially true for a moment of panic like this year. Even honest scientists, doctors, politicians, and public officials don’t have all the answers. But their bounded answers are much better than conspiratorial guesswork. Give doubt a chance.
B. Whom can we Trust?
Most Americans say that they trust major health agencies first 20 and that they are skeptical of their social media news feeds. 21 Are these intuitions justified?
My standard is to consider the sources’ incentives and capabilities:
Who is most willing and able to find the truth, the whole truth, and nothing but the truth?
By my values, research scientists must be at the top of this list, for at least two reasons. First, they are the only people with direct first-hand knowledge and expertise in the medical issues. Second, scientists are judged by how well they find truth, whether it’s beautiful or ugly.
There is a broad spectrum of media bias and credibility. I strongly recommend sites such as All Sides and Media Bias / Fact Check , which rank news sources on several criteria. Still, news outlets produce content for mass consumption, which requires them to simplify and / or sensationalize information. In an event like this pandemic, most news channels can only present a surface-level account – but it’s an essential first source.
I do not turn to politics for answers. This goes somewhat for office holders, but especially for party activists and armchair politicians. Partisans get emotionally attached to their parties’ preconceived notions. They then devote most of their time and energy to trash-talking each other and defending themselves. Truth takes a back seat to “who’s right” or, even more trivially, “who’s righteous”.
Social media rumors and word of mouth place lowest in my trust hierarchy. There are large but highly vocal segments of the population that lack the capacity or the incentive to manage voluminous, nuanced, complex information. Office holders, in turn, must pander to those folks for re-election.
Unelected government agencies in free countries are generally more trustworthy, as they are ideally sheltered from the partisan winds of emotionality. Agencies also have money for effective scientific and statistical research. Unfortunately, there is mounting evidence that President Trump has politicized US agencies like the FDA 22 , CDC 23 , and HHS 24 . Federal agencies have sent mixed signals as they have vacillated between public health advice and the president’s preferred messaging. 25
C. How Do We Feel?
“People are tired of COVID. People are saying, ‘Whatever, just leave us alone.‘ ” …
“You turn on CNN, that’s all they cover. ‘COVID, COVID, pandemic’ …
President Trump is describing crisis fatigue, aka chronic stress response. Whether we are stressed out about the virus itself, the economic impact, impositions on our lifestyle, or simply the unending arguments, most of us have felt stressed all year. Long-term stress is not natural, and it takes a toll on physical and emotional health. Nine out of ten Americans reported feeling emotional distress due to the pandemic, and that was already in May. 27
While a crisis can help unite people against a common enemy, in the long term it can aggravate political differences in addressing the problem. Other effects of chronic stress response include negative emotions and reckless behavior. 28 Substance abuse, crime, and suicide are running high in 2020. 29
Experts advise that knowledge is empowering to cope with stress. It is easier to confront facts than fears and rumors. It is also important to be aware of our own feelings. Only by identifying the sources and nature of our emotions can we ever hope to address them. Finally, look for solutions when you are in your best state. Let your “adult self” make your choices, not your “overwhelmed self” or your “survival self”. 30
Historians compare this pandemic to a depression or even a war that has potential to leave lasting changes in society. We know that billions of people have lived through such crises before – plagues, wars, tyrannies, and more. Most of us thought that we wouldn’t see such a catastrophe in our own lifetimes, but here we are. The classic stages of grief are denial, anger, bargaining, depression, and acceptance. History inspires us by proving that people can get through any tragedy when they learn to accept their new world.
D. How Should We Feel?
“Nobody panics when things go ‘according to plan’ even if the plan is horrifying!
Upset the established order, and everything becomes chaos.”
— The Joker, as written by Jonathan and Christopher Nolan, “Dark Knight” (2008)
In the politicized public discourse about coronavirus, one of the major through-lines has been the question, “How serious is this?” Should we feel afraid of the virus? Or is it no big deal? This deceptively simple question is difficult to answer even without the political complications.
One challenge is that we have to think as individuals and as a society at the same time. For you, as just one person, chances are slim (so far) that you’ll catch coronavirus, and slimmer still that it will make you seriously ill. But if we multiplied those small probabilities by the whole human population, we’d end up with tens of millions of preventable deaths. It comes down to a question of what you care about and what “we” care about.
Many people illustrate their perspectives by comparing the coronavirus pandemic to other causes of death. Other respiratory tract infections are a natural comparison. Diseases like tuberculosis, pneumonia, influenza, and COPD prematurely kill millions of people every year. 31 Why haven’t we been on red alert about them for decades? This is probably the hardest question I’ve encountered in my research. I posed this question to my Facebook friends early this year, and I still haven’t found a satisfactory answer. The only explanation I can conjure is the Joker’s principle, a psychological irrationality. Those diseases have reached equilibrium; they are part of the plan. They are known background noise, and it is the unknown that we fear. We don’t know how far or fast coronavirus will spread. Other dangers that alarm us and boil over in the streets, like terrorism or errant police brutality, kill miniscule numbers compared to any infectious disease. Our emotions are clearly not linked to the numbers.
When math nerds like me talk about uncertain events, we describe them with at least three components: Probability, costs, and benefits. You have to consider all three to arrive at the most rational way to quantify an event, its “expected value”:
E = P(B – C)
In a potentially dangerous situation, sometimes our mind exaggerates the probability P (like plane crashes). Sometimes we recklessly ignore a high cost or probability because we enjoy the benefit (like drugs). In the coronavirus situation, some people fixate on probabilities while others focus on the cost of death. This is why both sides can argue endlessly and both be partly right. A nuanced understanding must account for the whole formula.
In order to transcend irrational, emotional judgments, most regulatory agencies have adopted numerical limits to acceptable risks. The value of “one in a million” has become a widely accepted standard. 32 That is, if the probability of death is less than one in a million, a government will usually consider it unnecessary to commit further resources to controlling the risk. In a world of 8 billion people, this standard would set the acceptable threshold at 8,000 preventable deaths. We reached that point in March, less than a week after COVID-19 was recognized as a pandemic.
The premise that “coronavirus is just like the flu” is pretty accurate in terms of death toll so far. It’s the resulting conclusion that’s backward. This comparison does not demonstrate that the coronavirus is innocuous, but that influenza, like COVID-19, is vastly unacceptable.
IV. Conclusions
I am finishing this essay in the first week of November 2020, right in the middle of the Biden / Trump presidential election. I can’t imagine a more apt background. The coronavirus pandemic has loomed large in this election, both as an issue and as the environment in which we vote. Each party has a completely different vision of what the problems are and how to address them. Where Democrats see a serious public health threat, Republicans are not as concerned because it has not affected most of their personal lives. So far, preventive responses have been much more disruptive than the disease itself. Then again, it’s impossible to know how much worse the pandemic would have been without such measures.
Our perception of this pandemic is informed by politics and psychology as much as by facts. In complex controversies, one side rarely has all the answers. It’s not a matter of right or wrong but of emotional resonance. Different groups of people have different cares and concerns. It’s important to realize this, not only to manage your own thoughts but also to vet information and to understand your neighbors.
My next article will discuss solutions and a path forward.
Sara Burnett and Brian Slodysko, “Pro-Trump protesters push back on stay-at-home orders”, Associated Press (4/17/2020), https://apnews.com/ea4c17f541c7c63fac52941a6f43b885 (accessed, saved, and archived 9/23/20). ↩
Will Weissert and Jonathan Lemire, “Face masks make a political statement in era of coronavirus”, Associated Press (5/07/2020), https://apnews.com/7dce310db6e85b31d735e81d0af6769c (accessed, saved, and archived 9/23/20). ↩
Jonathan Haidt, The Righteous Mind: Why Good People are Divided by Politics and Religion, Pantheon (2012), Kindle edition around location 418 ↩
See e.g. V. Swami et al., “Putting the stress on conspiracy theories: Examining associations between psychological stress, anxiety, and belief in conspiracy theories”, Personality and Individual Differences vol. 99, pp. 72-76 (Sep., 2016), https://www.sciencedirect.com/science/article/abs/pii/S0191886916303440?via%3Dihub (accessed and saved 9/12/20). ↩
Olafur S. Palsson, Sarah Ballou, and Sarah Gray, “The U.S. National Pandemic Emotional Impact Report”, UNC and Harvard Schools of Medicine (6/29/2020), http://pandemicimpactreport.com/ (accessed, saved, and archived 11/03/20). ↩
“Pandemic”, the board game, was inspired by SARS. Now life imitates the art that imitated life.1
About This Primer
I am researching and writing this series to take a big-picture look at COVID-19. I’m taking a step back from the daily news information overload and fact-checking the (even larger) load of misinformation. I announced this project in June and invited questions from my friends. Part 1 covered the basics of viruses and coronaviruses. Part 2 dealt with SARS-CoV-2 on the level of individual health. Today’s article will be followed by Part 4, “Coronavirus and Society”.
In today’s installment, I start out with a discussion of COVID-19 data: how it is collected and what it can and cannot tell us. In section II, I discuss efforts to pin numbers on the virus to summarize this outbreak or compare it to others. Section III recaps the history of this pandemic and human responses to it in the first several months.
As you can imagine, no single agency could count every case, illness, or death. It’s a grassroots reporting effort. When you get your nose swabbed, your sample is sent to a lab for processing. Hospitals have labs as well as doctors who make personal diagnoses. Labs and hospitals report to local governments, which report to state or national governments. In the United States, the CDC issues reporting guidelines about who must report data, what they must report, and to whom. 2
Finally, national totals are reported to the World Health Organization for a global count. The most commonly reported vital statistics are the daily SARS-CoV-2-positive test results (“cases”), hospitalizations, hospitalizations requiring intensive care, and deaths. Private websites such as Johns Hopkins gather the data published by local and national governments. The data in most media articles will be drawn from a major consolidated database such as the COVID Tracking Project.
I have always felt partial to Worldometer. This website honed its census skills estimating real-time populations. 2It even has a stick-man graphic of all 8 billion people in the world, with births popping up before our eyes; see citation.3 Worldometer reports daily coronavirus figures for all US states and many counties, each nation, and the world. It explains its methodology to account for a lag in the reporting system. 4 Local counts are the most complete and current, so Worldometer relies on local data to supplement national information as much as possible.
B. Sources of Uncertainty
We could not possibly expect a decentralized, worldwide tabulation in a time of crisis to be 100% perfect. Some tests are more accurate than others. Cases might get lost or duplicated in the reporting system. The cases and deaths are usually categorized as “probable” or “confirmed.” 2A “probable death” means a death that was probably due to COVID-19. Changes or differences in these definitions can lead to disagreements between databases.
The greatest limitation of official data is that it only applies to reported cases. Since COVID-19 is mild for most people, and since testing hasn’t kept up with viral contagion, many infections will never enter the reporting system. Therefore, official records will under-report infections and over-report their death rate. This is a big topic that will be detailed further below.
Meanwhile, the death rate tends to be under-reported when we are tracking recent infections. For cases that are less than a month old, the data will show that they are non-fatal just because these patients haven’t died yet. While the number of infections continues to rise, a high percentage of cases are new and therefore unresolved. The most accurate death rates will come from the data of months past.
The point is not to conclude that official figures are useless. With numerous factors that both overestimate and underestimate reality, we can regard the reported numbers as middle-ground ballpark figures that are as precise as reasonably possible. Even if absolute figures are murky, they can still be useful for drawing comparisons across times and places. However, the most accurate information will not be available until the pandemic is over.
You may see references to an “excess deaths” statistic, which is appealing in its simplicity. The thought is that if we just count all deaths in 2020 and then subtract the baseline number of deaths in 2019, we will get the magic number of coronavirus-caused deaths. The excess death measurement was useful at the beginning of the outbreak before people had time to respond to it. However, this year’s social distancing and recession have affected death rates in so many other ways, such as the impact on accidents, medical practice, and other infectious diseases, that they drown out the impact of COVID-19 deaths. Excess deaths are no longer informative.
II. Viral Vitals
Reid S. asked, “Please determine the death rate!”
We are all anxious for clear-cut answers about this bug’s vital statistics. Unfortunately, if you want honest answers, you’re going to get complicated answers. Virtually every measure of a virus is impacted by human activity. The numbers vary greatly across time, place, and circumstance.
Some diseases are more contagious than others. The reproduction number, R, counts how many healthy people an average sick person will infect. The most disease-specific measure of R occurs at the very onset before people have time to respond to it. That value is called R0. The goal of preventive programs is to subdue R below 1 so that infections decrease. While R is above 1, even slightly, infections will continue to increase exponentially.
SARS-CoV-2 studies from Europe 5 and China 6 estimate R0 in the range of 2 to 9, most likely 4 to 6. This is much higher than seasonal flu, a little higher than SARS, and lower than chickenpox or measles. As of early August, R is estimated at 1.1 globally. Roughly half of the world’s countries are still above 1. The US has just reached R = 1, suggesting that this country is nearing its peak number of daily new infections. 7
B. Fatality Ratios
Brad B. asked about the impact of senior centers on death rates.
Of all reported cases of COVID-19 that have had time to run their course, 5% of them have been fatal as of mid-August. 8 The confirmed case-fatality ratio ranges from 0% in Vietnam (yep) to 15% in the UK! Singapore and other small countries like Qatar and the U.A.E. have young populations because they have large immigrant work forces. They are also rich countries with good hospital facilities. Despite major outbreaks, these countries have kept their death rates below 1%. The UK is a standout with its 15% case-fatality ratio. 9 The high British rate is largely due to slow and feeble government response to testing, tracing, and imposing public health standards. 10
By far the two most vulnerable populations are smokers and the elderly. Nursing homes are ground zero in this pandemic. With 1% of the US population, nursing homes report almost 25% of COVID-19 cases and 40% of its deaths. 11 Smokers are 14 times as likely as non-smokers to develop critical symptoms. 12 The death rate is higher in men than women. This pattern probably reflects the fact that most smokers are men.
C. Case-Infection Ratios
Brad B. asked, “What is the estimate of the number of asymptomatic and mild cases?”
Mitzi M-H. asked about the discrepancy between virus swabs and antibody tests
“Silent spreaders” are a big part of the COVID-19 story. The disease is contagious during an incubation period before symptoms appear. Many people carry the virus without ever knowing it. There is a great deal of interest in determining the “true” number of infections, for medical and political reasons alike.
The best way to detect whether a person has ever been exposed to a virus is with an antibody test. Although some antibody tests have had highly publicized flaws, there have been more reliable trials, and they yield a similar result. In April, lab analysis of randomly drawn blood samples estimated that there were about ten times as many infections as confirmed cases. 13 This ratio is variable too, as it depends on the quality and especially the quantity of swab tests.
Meanwhile, mathematical epidemiologists are working with the most reliable data (death toll and the best-measured infection-fatality ratios) and are running SIR algorithms to estimate the true number of infections. One sophisticated mathematical model in May estimated that infections are about four times more prevalent than reported cases worldwide, with a possible range of 2 – 12. 14
Many people argue that coronavirus is “less deadly than we thought” because of all the previously unreported infections that did not develop into serious cases. That is true in the sense of a death rate, although it obviously does not reduce the sheer number of deaths. In fact, the number of COVID-19 deaths is under-reported too, by a factor of up to 2. 15
Put it all together, and what do you get? I’ve done the math for you; you’re welcome. For a random person infected with the virus today, the probability of death is probably closer to 1% than 5%. Whatever that means for your peace of mind is up to you!
The good news is balanced by bad news anyway. The large pool of untested infections means that for every case that is followed up with quarantine and contact tracing, there are about ten others who go undetected. This highlights the need for much, much more testing, and not just for sick people.
By the way, even accounting for the unreported infections, still only about 1% of the human population has the antibody. We’d need a prevalence of about 80% for herd immunity. 16 Letting the disease play itself out to herd immunity would therefore multiply the death count by 80, to about 50,000,000. Needless to say, that’s an unacceptable solution.
Like many social ills – poverty, crime, overpopulation – the impact of COVID-19 is not distributed evenly throughout the world but is spotty. It has devastating impact on a few localities like dense cities and senior centers. In those localities, it hits the weakest links in the medical supplies and services chain.
When WHO declared COVID-19 a global health emergency on January 30, the disease had killed only 200 people. If those deaths had been spread around the world, nobody would have noticed. They would have been a drop in the bucket of 5,000,000 normal deaths that month. But those deaths, as well as 10,000 non-fatal cases, were concentrated around one city. Wuhan probably could have handled them if they had been spread out over a year. It was the concentrated impact of 10,000 cases in one city in one month that was so exceptionally stressful. Wuhan hospitals were so short on beds and ventilators that the government erected a new hospital in two weeks. Similar stories of overwhelmed resources occurred in Milan, Tehran, and New York City by early March. Ventilators were the scarcest need. Not every hospital has them; some countries have only a few. 17 By March, demand was already ten times the global supply. 18 Making new ventilators requires a massive global supply chain; it’s not easy to crank them out. 19 Medical personnel and ICU beds are other resources that got exhausted quickly.
B. Effectiveness of Social Measures
Brad B. asked if there has been a change in the hospitalization rate.
The early urban hotspots were warnings. If left to spread out of control, the virus had the potential to strike every city like that eventually. WHO upgraded the disease to a pandemic on March 11, and governments around the world took measures shortly afterward. This led to some enlightening experimentation. Two countries that had exemplary success curbing COVID-19, South Korea and Iceland, did so by immediately implementing rigorous programs of testing, contact tracing, and quarantining. Iceland finished assembling its coronavirus task force literally hours before the country’s first reported case. 20 Meanwhile, China and Italy each put 60,000,000 people on lockdown. Italy’s outbreak has been on a steep decline since late March. China enforced its lockdown more strictly, and its wave was effectively over before Italy’s began.
Facemasks and social distancing have been effective at slowing the spread everywhere and bringing it under control in half the world. Masks reduce transmission by up to 50% when used widely. 21 The countries that see masks worn most faithfully, in Asia, have low transmission rates. 22 Without any mitigating behavior, this virus could have infected 7,000,000,000 people and killed 40,000,000 this year. 23 Good job, us!
The number of daily deaths took a significant dip in April despite rising case counts. 24 This can’t be explained away with rates or miscounts, so it seems to reflect genuine improvement in public health. Maybe defenses got tightened up at nursing homes or the most vulnerable people got more serious about staying home. Perhaps doctors learned from experience, or hospitalizations got spread out more evenly across geography and time.
Global data showing the impact of human activity after March 11, when WHO declared COVID-19 a pandemic. Note how the “Daily New Cases” curve slows down abruptly around March 30, and “Daily Deaths” plummet around April 16.
The biggest problem this year has been lack of preparedness, coordination, and resolve. That is showcased by the approaches of the United States, United Kingdom, and Sweden. These are countries that like to flout government orders, 25 and their governments were slow to acceptance anyway. Now, the US has the world’s largest case load, the UK has the highest death rate, and Sweden has one of the highest reproduction numbers.
However, very few countries were as prepared as they should have been. A 2019 study ranked countries on their pandemic preparedness. Its report card gave a global average of 40%. 26 “Few countries pay for action plans out of national budgets,” the report found. That explains why everybody had to scramble to legislate aid packages this year.
Africa’s fate is one of the greatest unresolved questions. Although many African nations are woefully unprepared, so far, numbers are low across the continent. This is correlated to low testing, but the case-fatality ratio is low too. Africa is the youngest continent, so it could be that its population is truly resilient. 27 Cases are just starting to blow up in a few hotspots like Congo, Djibouti, and South Africa.
2. Reopening
Lockdowns cannot continue forever. However, when full mobility resumes, this pandemic will start all over again, a “second wave”. The only way to get the outbreak under control without a vaccine is to continue lockdowns until new cases are reduced to a trickle, then have a testing / tracing / isolation system ready at the starting line when the economy reopens. 28
We face challenges this fall as schools resume, pneumonia season begins, and sectors of the economy simply must reopen out of necessity. The hope is that we’ll be more prepared this time. Let’s hear it for second chances.
Kevin Linka, Mathias Peirlinck, and Ellen Kuhl, “The reproduction number of COVID-19 and its correlation with public health interventions”, medRxiv (submitted 5/01/2020, peer review in progress), https://www.medrxiv.org/content/10.1101/2020.05.01.20088047v3 (accessed and saved 8/03/20). ↩
Steven Sanche et al., “High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2”, Emerging Infectious Diseases 26(7):1470-1477 (Jul., 2020), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7323562/ (accessed and saved 8/04/20). ↩
Garegin Papoian et al., “The Covid-19 Accelerometer Dashboard: World Statistics of Rt (Effective Reproduction Number) (continuously updated), https://covid19-r0.com/ (accessed 8/04/20). ↩
Global Worldometer data as of 8/16/20: Out of 15.6 million closed cases to date, 777,000 have resulted in death. ↩
See e.g. staff writer, “Commercial Laboratory Seroprevalence Survey Data”, US CDC (last updated 7/21/2020), https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/commercial-lab-surveys.html (accessed 8/05/20). A survey of samples from ten US sites found actual infections mostly 6 – 12 times more prevalent than previously reported cases, with an outlier at 24 times. ↩
Christina Bohk-Ewald, Christian Dudel, and Mikko Myrskyla, “A demographic scaling model for estimating the total number of COVID-19 infections”, medRxiv (5/26/2020), https://www.medrxiv.org/content/10.1101/2020.04.23.20077719v3 (accessed and saved 7/28/20). ↩
For most of us, 2020 is a year of masks, gloves, temperature checks, and social distancing. 1
I began this series with background information, zooming in from the domain of viruses to the genus of coronaviruses. Today’s post specifically introduces this year’s novel coronavirus. We’ll cover the topics of the virus’s origins and evolution, its effects, person-to-person transmission, and possibilities for a cure. Part 3 (next month) will discuss the effects of this pandemic on populations and society.
The current pandemic is the third wave of deadly human coronavirus infections. The new virus is officially called SARS-CoV-2, and the disease that it causes is COVID-19. COVID simply stands for COrona VIrus Disease.
This year’s virus is so closely related to the 2002 SARS virus that virologists classify it as a new strain of the same species. 2 SARS-CoV-2 is not a descendant of SARS-CoV but a “cousin” that shares a recent common ancestor. Though conspiracy theorists will believe what they will, genetic evidence shows with high confidence that the SARS-CoV-2 virus evolved naturally and was not engineered in a lab. 3
The path of transmission, from bat to intermediate host to human, is uncertain. The pangolin or “spiky anteater” was an early prime suspect because pangolins carry a coronavirus similar to SARS-CoV-2. The current human and pangolin coronaviruses turned out to be, again, only cousins. 4 Nevertheless, they are similar enough to raise concerns about pangolins as potential carriers for future outbreaks, especially since the pangolin is a heavily trafficked wild animal.
The earliest confirmed human case of SARS-CoV-2 was reported on November 17 in Hubei Province, China (where Wuhan is located). 5 Interestingly, traces of the virus have been found in samples collected from Europe in December. One was in Italian wastewater 6 and another in the bodily fluids of a French man who was tested for pneumonia. 7
The first mass outbreak came in late December. It was traced to the Huanan Seafood Wholesale Market in Wuhan, China. Because the market sells exotic animals, and because similar markets had been implicated in zoonotic transmission of SARS, people quickly jumped to the conclusion that Huanan Market was the site where the virus made its first jump into humans. However, we now know that some early cases were not associated with Huanan Market 8 and that none of the animals at that market were infected. 9 It seems that a person who already had the virus brought it to the market, and it spread simply because of the crowded conditions. The spike in Wuhan hospitalizations started to make headlines right around the first day of the decade.
B. Evolution
Taletha D. asked: “How many versions are there? How fast did they mutate? Why might they have mutated?”
After SARS-CoV-2 infected people, its evolution was then guided by its human cell environment. The virus has at least two variants, the “G” and “D” varieties. They differ by only one “letter” in their RNA code, but the G version is much more effective at latching onto human cells. 10 Hence, the virus has been evolving strongly toward the G variety this year, especially in Europe and the United States. Unfortunately for us, G’s gain is our loss. The G virus is ten times as transmissible as D. In other words, a sneeze requires only 10% as many G viruses as D viruses in order to spread equally to people nearby. This explains why the epidemic is spreading through the US more rapidly than through China.
Mutations, or genetic changes, happen randomly. The G and D varieties might even have existed before human infection. The part that’s not so random now is the evolution, the competition between G and D in human cells. Since G is so much more effective, it will come to dominate the viral population.
Taletha D. asked: “Why are some people asymptomatic?”
Karen K. asked, “I’m interested in the research on long-term kidney and lung damage.”
Individuals display a tremendous range of responses to SARS-CoV-2 infection. The typical manifestation is normal flu-like symptoms. Some patients experience severe symptoms like shortness of breath, low blood oxygen, or moderate pneumonia. The most critical cases involve respiratory failure, shock, or multiorgan system dysfunction, 11 which can of course be fatal. Some of the damage comes from the virus itself, and some from cytokine storm, the immune system’s overreaction. On the other extreme, some cases present no symptoms or signs at all. 12 The percentages of these categories are still in flux, and will be discussed further in Part 3.
The spike protein of SARS-CoV-2, like its cousin SARS-CoV, binds to a protein called ACE2. ACE2 is distributed unevenly in the human body. It is present in our lungs, heart, blood vessels, kidneys, liver, GI tract, and the lining of the mouth and nose. Early COVID-19 reports show that damage to the heart, kidneys, and liver are a serious concern in the worst cases. 13 However, ACE2 is more abundant in the lungs, and that’s where the worst impact will be. 14 Even some asymptomatic carriers get lung damage! 15 The lining of the nose is especially rich with ACE2. 16 That explains those highly invasive nose swabs. The only true long-term data we have is from SARS-CoV. A small percentage of SARS survivors suffered long-term lung and kidney damage. Fortunately, most have recovered completely. 17
The severity of symptoms is correlated to the intensity of viral infection as well as underlying medical factors. Those with the most critical symptoms tend to be those who had pre-existing conditions commonly associated with old age, obesity, and smoking. 3The CDC lists about 20 factors. Most of them are correlated to old age, obesity, and / or smoking. The truly independent conditions are much rarer. See citation.18 We still don’t know why some people don’t develop symptoms at all.
The long-term immune response is another great unknown. We know that the human immune system synthesizes antibodies; almost 30 varieties are currently cataloged. 19 We haven’t had enough time to tell how long a SARS-CoV-2-specific antibody will remain in a survivor’s bloodstream. As a reasonable comparison, SARS survivors maintained SARS-CoV-1 antibodies in their systems for an average of two years, with significant reduction after three years. 20 Preliminary results seem to show that SARS-CoV-2 exhibits a similar pattern. 21 If so, then we might have to rely on annual shots to avoid getting overwhelmed by future outbreaks.
B. Transmission
Julie W. asked if (and why) food really presents lower risk than surfaces.
SARS-CoV-2 is almost entirely transmitted directly from person to person through exhaled airborne water droplets. Factors that increase transmissibility include the concentration of virus in a sick person’s system, proximity, crowd density, and duration of contact. The six-foot rule is based on the distance that the largest cough / sneeze droplets will travel. This distance is also chosen as a reasonable compromise between medical precaution and social necessities. However, the dynamics of a sneeze are startlingly effective at spreading germs far and wide, especially because “sneeze clouds” tend to rise and get picked up by ventilation systems. 22
The virus usually incubates in a person for a day to a week before onset of symptoms. Contagion peaks from two days before to two days after the onset of symptoms. 23 Although we hear a lot of debate about asymptomatic spread, the greater concern is in fact presymptomatic spread. Of course, someone without symptoms doesn’t know whether she’s uninfected, asymptomatic, or presymptomatic until she starts coming down with symptoms, when it is too late to prevent transmission. After she develops symptoms, she may be contagious for another week, 24 but by that time she knows she’s sick and is more likely to be quarantined. The recommended two-week quarantine period comes from adding a week of incubation plus one more week of contagion.
The makeshift face masks that we ordinary people wear out in public are meant to minimize the spread of water droplets from our own mouths. These masks protect those around us (in case we are presymptomatic). No, they are not 100% cough-proof, but they are pretty effective at slowing down water droplets 25 and reducing microbial spread. 26 The respirators reserved for medical workers are engineered for nearly complete two-way filtering; they protect doctors and nurses from infected patients.
We are often warned about touching things – surfaces, other people’s hands, or our own faces. These are secondary precautions against indirect transmission. The pathway here is that a sick person coughs or sneezes, his viruses land on a surface (which might be his own hand), a healthy person touches that surface and picks up the virus, and then the healthy person touches her face. The virus doesn’t penetrate skin, but the eyes, mouth, and nose are vulnerable points of entry. Since viruses don’t last long on surfaces, they don’t spread as readily this way. That’s why gloves are not mandated nearly as much as face masks and distancing.
Best-practice signs in Los Angeles, CA, 6/24/20. 27
The virus can remain on some surfaces for up to three days, though not in great numbers. 28 An exposed surface is not a hospitable place for a virus, so the risk is proportional to how often people touch the surface. It’s a safe bet that many more people have handled the subway pole than your Subway sandwich!
Since viruses don’t “eat”, food to them is just another surface. They could theoretically infect bacteria on the food, but that is not a good route for viral proliferation. It’s not likely that SARS-CoV-2 would find the right receptors in bacteria cells anyway. There have been no known reports of people catching COVID-19 through food packaging. 29 Although the virus could theoretically live on produce, that has not been demonstrated as a known vector either. 30
Over 40 vaccine trials are in progress. 31 Vaccine development, testing, and approval is an arduous process that normally takes a decade. Testing occurs in three phases, with a larger and more vulnerable cohort in each phase. Regulatory agencies are now permitting “fast track” approval processes that could theoretically accelerate the SARS-CoV-2 process to as short as 1 – 2 years. This would be an unprecedented pace.
The United States’ Operation Warp Speed is a major collaborative vaccine effort between the federal government and private labs. OWS has selected three top contenders for Phase 3 testing this summer. All three teams – Moderna 32 , Oxford / AstraZeneca 33 , and Pfizer / BioNTech 34 – have reported encouraging results in their Phase 1 trials. The Oxford vaccine is especially promising because it stimulates T cells, special white blood cells that would last longer than antibodies.
The road ahead is not guaranteed to be smooth and easy. Some of the leading competitors in this race, including Moderna and Oxford, have never commercialized a vaccine before. Proper dosages are still unknown. The sterile plastic vials that contain vaccine doses will be a major bottleneck in distribution. 35 Nevertheless, these firms continue to speak optimistically of vaccine production beginning this year.
2. Antiviral
There are five or ten viable candidates for anti-coronaviral medications. Most of them were created years ago for other viruses. Antivirals are known to have strong side effects, so they are usually reserved for the worst cases until they’ve had adequate testing to prove them safe.
One of the most promising drugs is called remdesivir, by Gilead. This was a failed candidate for treatment of Ebola. One trial has shown that it appreciably reduces the recovery time for surviving patients hospitalized with COVID-19. 36 The FDA has now issued Emergency Use Authorization for remdesivir to treat severe cases. 37
Eli Lilly has taken a new approach to an old remedy, the old “antidote from a survivor’s blood” trick. After drawing antibodies directly from the blood of a COVID-19 survivor, this company formulated them into a medication called LY-CoV555. It has been effective in the lab, and is currently being tested on human subjects. 38
3. Symptomatic treatments
The worst cases of COVID-19 result in low blood oxygen and inflamed air passageways. Ventilators, highly invasive and cumbersome machines, have been the last resort in this fight. Ventilators present numerous problems of their own. They can infect patients and damage lungs. Intubating a patient can eject virus-infected bodily fluid into the air, endangering healthcare workers. It turns out that COVID-19 patients have surprisingly high tolerance for low blood oxygen. Researchers now recommend simpler devices such as oxygen tanks and even CPAP machines for patients who have low oxygen as long as they’re still breathing comfortably. 39
Dexamethasone, an anti-inflammatory medication, is the first drug proven to save lives of coronavirus patients. It was already a well-known pharmaceutical before this pandemic. Encouragingly, it is also inexpensive. It has now been shown to reduce the death rate of critically ill patients by 20 – 30%. 40 However, it has not been properly vetted for side effects, and is not recommended for mild cases. Researchers are cautiously optimistic.
Hydroxychloroquine is a 1950s medicine made controversial when touted by President Trump. It has been effective against malaria and lupus, neither one of which is caused by a virus. It also has anti-inflammatory benefits for treating arthritis. It showed early promise at reducing SARS-CoV-2 in petri dishes (though nobody knew why). Clinical trials in humans have been inconsistent. 41 Hydroxychloroquine actually appears to suppress the initial immune response against SARS-CoV-2 42 , and it can be harmful to vital organs. 43 The FDA and WHO have dropped it from consideration.
4. Cocktails and computer-aided concoctions
Why choose just one? The strongest remedies could turn out to be hybrids or pharmaceutical “cocktails”, as for AIDS. Roche and Gilead are conducting a trial to combine remdesivir with an anti-inflammatory; expect Phase 3 results this summer. 44 Carprofen and Celecoxib are anti-inflammatories that also appear to slightly inhibit replication of SARS-CoV-2. 45
The latter two drugs were identified by computerized analysis of pharmaceutical databanks. A crowdsourcing project is underway to identify, synthesize, and test more super-candidates like these. The world’s top chemists are submitting their ideas, and new supercomputer lab PostEra is running simulations to see if and how they can be made. PostEra has pledged to release any winning chemical formulas into the public domain. When I first read about this, I called it a “global brainstorm.” PostEra has a better name for it: “COVID Moonshot”. 46
Alexandar E. Gorbalenya, “The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2”, Nature Microbiology 5, 536-544 (3/02/2020), https://www.nature.com/articles/s41564-020-0695-z (accessed and saved 7/23/20). ↩
From a sample of animal tissues at the market by the Chinese CDC and / or Wuhan Institute of Virology. I have not yet seen the original report, but it was published shortly before 5/26, when the Wall Street Journal reported on it. The Chinese report was vetted by American scientist Colin Carlson, who finds its results credible. Carlson communicated the report to LiveScience. See excellent summary at Rafi Letzter, “The coronavirus didn’t really start at that Wuhan ‘wet market’”, LiveScience (5/28/2020), https://www.livescience.com/covid-19-did-not-start-at-wuhan-wet-market.html (accessed 7/03/20). ↩
Heng Meng et al., “CT imaging and clinical course of asymptomatic cases with COVID-19 pneumonia at admission in Wuhan, China”, J. Infect. 81(1):e33-39 (4/12/2020), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7152865/ (accessed and saved 7/04/20). ↩
Waradon Sungnak et al., “SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes”, Nature Medicine 26, 681-687 (4/23/2020), https://www.nature.com/articles/s41591-020-0868-6#Fig1 (accessed and saved 7/14/20). ↩
Li-Ping Wu et al., “Duration of Antibody Responses after Severe Acute Respiratory Syndrome”, Emerging Infectious Diseases 13(10):1562-4 (Oct., 2007), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2851497/ (accessed and saved 7/19/20). ↩
Quan-Xin Long et al., “Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections”, Nature Medicine (6/18/2020), https://www.nature.com/articles/s41591-020-0965-6 (accessed and saved 7/21/20). ↩
The facts about incubation and contagion are taken from Xi He et al., “Temporal dynamics in viral shedding and transmissibility of COVID-19”, Nature Medicine (4/15/2020), https://www.nature.com/articles/s41591-020-0869-5 (accessed and saved 7/19/20). See esp. fig. 1c. ↩
Neeltje van Doremalen et al., “Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1”, New England Journal of Medicine 382:1564-1567 (3/17/2020), https://www.nejm.org/doi/full/10.1056/nejmc2004973 (accessed and saved 7/14/20). ↩
Lisa A. Jackson et al., “An mRNA Vaccine against SARS-CoV-2 – Preliminary Report”, New England Journal of Medicine (7/14/2020), https://www.nejm.org/doi/full/10.1056/NEJMoa2022483 (accessed and saved 7/20/20). ↩
Amy Rose et al., “Pfizer and BioNTech Announce Early Positive Data from an Ongoing Phase ½ study of mRNA-based Vaccine Candidate Against SARS-CoV-2”, Business Wire (7/01/2020), https://www.businesswire.com/news/home/20200701005576/en/ (accessed, saved, and archived 7/20/20). ↩
Ardan M. Dondorp et al., “Respiratory Support in COVID-19 Patients, with a Focus on Resource-Limited Settings”, Am. J. Tropical Medicine & Hygiene 102(6):1191-7 (6/03/2020), https://www.ajtmh.org/content/journals/10.4269/ajtmh.20-0283 (accessed and saved 7/21/20). ↩
Nicholas Dunant et al., “Roche initiates phase III clinical trial of Actemra/RoActemra plus remdesivir in hospitalized patients with severe COVID-19 pneumonia”, Roche (5/28/2020), https://www.roche.com/media/releases/med-cor-2020-05-28.htm (saved, accessed, and archived 7/22/20). ↩
Aleix Gimeno et al., “Prediction of Novel Inhibitors of the Main Protease (M-pro) of SARS-CoV-2 through Consensus Docking and Drug Reposition”, Int’l Journal Molecular Sciences 21(11):3793 (5/27/2020), https://www.mdpi.com/1422-0067/21/11/3793 (accessed and saved 7/22/20). ↩
Alpha Lee et al., “COVID Moonshot: Help Us Fight Coronavirus”, PostEra, https://postera.ai/covid (accessed, saved, and archived 7/22/20). ↩
Without a doubt, the biggest story of 2020 is the coronavirus epidemic. 2I personally prefer to spell “corona virus” with a space, as I generally prefer to err on the side of spaces to make compound words easier to read, but the consensus is against me. By the middle of the year, I, like many others out there, felt overwhelmed in a muddle of fragmented news and science, misinformation, and general confusion. I announced on Facebook that I wanted to “digest it all” and assemble the best known information into one primer. “Any questions you’d like me to research?” I asked, and a few friends immediately chimed in with requests. Hopefully, this will help us understand coronavirus basics from the ground up. I will begin this primer with the big picture and then gradually zoom in from viruses to coronaviruses to this year’s unwanted pests. There is far too much ground to cover in one article, so I’m breaking it into multiple parts. Today’s post is Part 1: Background. This article discusses viruses and coronaviruses in general.
Viruses occupy one of the most intriguing positions in the whole grand scheme of things. They are microbes right at the boundary of life and non-living chemistry. This makes them primary subjects of interest for scientists studying the origins of life.
You are made of about 30 trillion cells. 2 We call a cell the smallest unit of life because it performs all the functions that we expect of a living thing. A cell grows, responds to stimuli, metabolizes, heals, sustains and defends itself, reproduces, and dies. However, it is not a unitary blob of spittle. A cell is a complex system with hundreds of interacting parts, with names like macromolecules and organelles. Most of those parts specialize in just one life function, so by themselves they are not fully alive. If I could compare a virus to anything else, I’d say it’s like a cell organelle that specializes in reproduction.
Viruses are like living things in numerous ways. They are made of the same basic macromolecules as us: nucleic acids, proteins, lipids, and carbohydrates. At the core of every virus is a bundle of DNA or RNA comprising a few genes. Viruses reproduce and evolve / speciate. Biologists classify them and give them Latinesque scientific names. Viruses can be “killed” by heat, chemicals, or radiation.
However, viruses are like lifeless chemicals in that they don’t metabolize, respond, heal, change, or grow. Nor are they able to protect themselves from the environment. And although viruses specialize in just one thing – reproduction – they can’t even do that by themselves. A virus is an absolute parasite. In order to function, it must inhabit a living cell. The “life” cycle of a virus is to invade a cell and exploit the cell’s resources to make dozens of copies of itself, which then burst forth to invade other cells. Viruses infect the cells of all living things, from bacteria to whales. They kill more life forms, and more humans, than any other force of nature.
B. Infection, Immunity, Inoculation
While some viruses are harmless or even beneficial, most of them cause irreparable or fatal damage to their host cells. Rapidly reproducing viruses consume a cell completely and then burst out like a battalion of creepy little microscopic robots. Since they are vulnerable outside of cells, they must pass quickly from dying cell to living cell. They can pass from one person to another through skin, body fluids, or air currents.
Viral infection involves proteins on the surfaces of viruses and cells. Proteins have complex three-dimensional shapes like locks and keys. If a virus has the protein “key” to a cell’s outer “lock”, it will latch on and inject its genes inside.
In a human or animal body, fragments of viruses called antigens react with our white blood cells, aka our immune system. In lucky cases, the immune system produces a protein called an antibody, a natural defense. An antibody latches onto the antigen that stimulated it. Sometimes, the antibody disfigures the virus’s “key” so that the virus can no longer penetrate cells. Other antibodies “flag” a virus so that white blood cells can easily identify and destroy it. While a person has an antibody in his blood, he is immune to that virus. The next time the virus comes along, his antibodies will latch onto the virus’s antigens and slow it down or stop it. Some antibodies last a lifetime, while others disappear from the bloodstream in a few years. A vaccine is a human-made, finely tuned dose of antigens – just enough to stimulate an immune response without a full-blown infection. If enough people in a community become immune to the virus, whether through natural immunity or vaccine inoculation, the virus begins to die out and can even go extinct.
It’s important to note that viruses evolve quickly. This is especially true of RNA viruses, which most human viruses are. When a virus evolves, its proteins can change shape. That is a headache for us; we are forced to keep reinventing new locks to morphing viral keys. Occasionally, a virus that infects one animal will evolve to a new form that infects another animal, including humans. A virus that jumps ship from one species of host to another is called zoonotic.
C. Human Viral Diseases
A viral disease is not quite the same as the virus that causes it. A disease is the physical manifestation of the virus, its effects on the person. Sometimes a virus and its disease have different names, as HIV (Human Immunodeficiency Virus) causes AIDS (Acquired Immuno-Deficiency Syndrome). In other cases, we use a single term, like “Ebola”, to name both the virus and its disease. There are too many human disease-causing viruses to list here. Examples include adenoviruses, astroviruses, encephalitis, enteroviruses, hepatitis, herpes, HPV, influenza, measles, meningitis, mumps, noroviruses, parainfluenza, polio, pox, rabies, rhinoviruses (which cause colds), roseola, rotaviruses, rubella, West Nile, Zika, … you get the picture.
D. Measuring Epidemics
Viruses are inherently public health threats. Human viruses would quickly die out if they did not have lots and lots of people to infect. Viral infections can be quantified in numerous ways. The three most fundamental independent metrics are reproduction number, transmission time, and case-fatality rate.
Reproduction number is commonly abbreviated as R0. It measures the average number of healthy persons who catch the virus from each infected person. For example, if each sick person makes four other people sick, then R0 = 4.
Transmission time is the average time it takes a virus to spread from one person to another. I don’t see this factor discussed very often, but it makes a big difference whether a sick person infects others in a matter of hours (like an airborne virus in a mall) or years (like a sexually transmitted virus).
Finally, the infection-fatality rate is the most morbid statistic of them all: the percentage of infected persons who die. The number of serious illnesses or hospitalizations may be measured as well; they will be closely correlated to the fatality rate.
Unfortunately, the fundamental metrics above are difficult to measure. We can’t measure them all in a lab because they are not entirely intrinsic to the virus. They depend on human activity too. It’s hard to know how many people are infected when not everyone is tested and / or exhibiting symptoms.
The easiest way to measure the severity of an epidemic is with the number of deaths and / or hospitalizations. These numbers are documented well. There will still always be some over-reporting (deaths attributed to the virus that were really due to something else) and under-reporting (deaths due to the virus that weren’t counted). On a societal level, sheer numbers are more meaningful than rates. It doesn’t really matter if there are 1,000 infections that are 10% fatal or 10,000 infections that are 1% fatal. Both scenarios will result in 100 deaths and should be considered equally dangerous. Of course, if you get infected, you sure will be interested in knowing if you have a 1% or 10% chance of dying!
Taken together, the reproduction number and transmission time determine the doubling time, or the amount of time it takes for the prevalence of infections to double in the population. The pattern characterized by a constant doubling time is called exponential growth. In real life, exponential growth never lasts long, because it runs up against limitations like immunity or finite populations. Doubling time is the metric we hear most on the news, because it is easy to calculate by simply counting cases. Breaking it down offers slightly more insight, if only theoretically. When doubling time increases, it demonstrates that each sick person is infecting fewer healthy people and / or she’s doing so more slowly, which are the intended effects of social distancing.
When doubling time slows down (as it always must) the simplest model for epidemic growth is the logistic formula. This S-shaped curve represents the all-time number of cases “flattening” as it reaches its maximum and stops growing. The point where the number of daily cases starts to decrease is the point of inflection. I hear some people using the term “inflection point” as if it means the point where a virus “really takes off”. That’s the opposite of the correct meaning, and there is no well-defined point of acceleration on the curve.
Real epidemiologists use sophisticated numerical algorithms that model the interactions among Susceptible, Immune, and Recovered people. These SIR or compartmentalized models are run on supercomputers.
The logistic curve, unlike exponential growth, models the “flattening” or maxing out that must eventually occur. The inflection point is where growth starts to slow down; it is shown at (5, 50) on this example.3
E. Treatment Options
Besides vaccines, there are at least two medical options for some viral infections.
Antiviral drugs kill viruses after infection. Antiviral pharmacology is recent technology. It is more sophisticated than vaccinations. To produce an antiviral medicine, researchers sequence the virus’s RNA and proteins and then engineer molecules to target the virus’s vulnerable points. This highly advanced research developed in response to the AIDS pandemic.
Each vaccine or antiviral medication is engineered specifically for one strain of virus. Though the vaccines for polio and smallpox were “miracle cures” that drove their viruses to extinction, they are useless against other viruses. Medical labs are experienced and pretty effective at making influenza vaccines. On the other hand, centuries of effort have still yielded no rhinovirus vaccines.
Because vaccines and antivirals are not always available, hospitals must also rely on symptomatic treatments, which only mitigate the disease without managing the virus. Some drugs treat symptoms such as inflammation (also known as cytokine storm). In extreme cases, medical equipment like ventilators assist with breathing while the virus passes.
Coronaviruses are classified as the family Coronaviridae in the virus family tree. They get their name from the “spike” proteins, also known as S proteins, embedded in their fatty envelope. The spikes look like the corona (crown) of the sun, and they are the killer proteins involved in latching onto host cell membranes.
Coronaviruses have infected bats and birds for tens or hundreds of millions of years. 4 They are occasionally transmitted to other mammalian species that come into contact with bats. There are now five genera of coronaviruses. Two of them, Alphacoronavirus and Betacoronavirus, include species that infect humans. Today’s living alpha- and beta-coronaviruses descend from a common ancestor four or five millennia ago. 5
Some animal diseases that are now recognized as coronavirus infections came to veterinary attention in the early 20th century. The viruses themselves were only observed and named in the 1960s. Since then, the medical community has identified seven coronaviruses that infect humans. Four of them only cause colds. The three most recent strains, all beta-coronaviruses that evolved in the 21st century, are much more severe. There are no known treatments for any of them.
B. The First Two Killer Coronaviruses
The first alarming coronavirus outbreak was the SARS epidemic of 2002 – ’04. SARS stands for Severe Acute Respiratory Syndrome. 2I thought this phrase was redundant, but acute doesn’t mean “severe”. It means “occurring once or suddenly”, the opposite of chronic. The virus that caused it was named SARS-CoV. The SARS coronavirus originated in horseshoe bats in southern China. 6 It was then apparently transmitted to intermediary species that were sold in exotic animal markets: the palm civet (a wild cat), the raccoon dog (a wild dog), and / or the ferret badger. All of these species carried SARS-CoV-like viruses. The exact pathway from bat to carrier to human has not yet been solved.
SARS had a high case-fatality rate, about 10%. It was easy to detect infected people, though, because almost everybody who caught it broke out into fever and coughs within 2 – 3 days. The sick were quickly quarantined and questioned about their most recent contacts, who were also isolated. Local governments also ordered a mass killing of palm civets. 7 Even without a vaccine or anti-viral remedy, the anti-SARS campaign was a complete success. Only 8,000 people ever caught this disease. Canada was the only non-Asian country with more than one death. Curiously, just like COVID-19, SARS barely touched Africa. The peak of the outbreak lasted just a few months, February – July 2003. The onset of summer weather slowed it down. By 2004, SARS-CoV was extinct.
Living in a world city, Los Angeles, I have long noticed Chinese nationals wearing face masks all the time, and I always wondered why. It’s the SARS outbreak that got them in the habit, and many have worn masks routinely ever since 2003. It doesn’t seem so unusual anymore!
The next major coronavirus outbreak was called MERS (Middle East Respiratory Syndrome) because it was concentrated in Saudi Arabia and neighboring countries. The MERS virus passed from bats to camels in the 1990s and then to people who made close contact with camels in 2012. This virus had a distinct profile. MERS had a much higher case-fatality ratio. 30 – 35% of the patients who caught it died! Fortunately, it did not easily pass from one person to another. The MERS virus still exists, but it has only killed 900 people, just a few each year now.
In 2017, the scientists who traced SARS-CoV to a bat cave in Yunnan Province observed that the viruses were recombining (intermixing) to form myriad new combinations. Their discussion included this prophetic warning:
“We have also revealed that various SARSr-CoVs … are still circulating among bats in this region. Thus, the risk of spillover into people and emergence of a disease similar to SARS is possible.” 8
Patrick C.Y. Woo et al., “Discovery of Seven Novel Mammalian and Avian Coronaviruses in the Genus Deltacoronavirus Supports Bat Coronaviruses as the Gene Source of Alphacoronavirus and Betacoronavirus and Avian Coronaviruses as the Gene Source of Gammacoronavirus and Deltacoronavirus”, Journal of Virology 86(7):3995-4008 (Apr., 2012), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3302495/ (accessed and saved 6/25/20). ↩
I recently announced a quest to find the most “profitable” places to be self-employed. I am posting my deliberations online in case others might be interested in my thought process and / or findings.
As I started researching various locations, I found that my initial model of “Median Income – Median Rent” was a little too simple to capture the realities of living in one place vs. another. The hard part is estimating how much I’d earn. For instance, some of the wealthiest neighborhoods are sparsely populated, so it’s hard to see how I’d pull in good business there. This has forced me to take a closer look at what I need in a locale. That, in turn, depends very much on the services and clientele that I serve. Before I can get much further, I need to take a closer look at myself and my needs. This analysis will have very different details for each businessperson, but the same principles will apply: Define your market households and find out where they are.
My Services
I run a unique shop as a tutorney: part tutor, part attorney. A look at last year’s bookkeeping reports showed me how last year’s revenue was distributed across three categories of service. The breakdown was pretty close to:
Legal and patent services = 50%
One-on-one tutoring = 25%
Group classes = 25%
Before I looked it up, I didn’t even know this basic fact. I’m learning something already! Thus far, I need all three streams of income to make a living.
My Market Households
To complicate matters, these services cater to different demographics.
My core clientele for legal and patent services is small businesses and mid-to-high income individuals, so let’s say the market household is $100,000+ income. Clients call into my law office from a fairly broad region of the Los Angeles metropolitan area, mostly within, say, a 25-mile zone. It wouldn’t make much of a difference where my law office is located within a city. It’s the city that will make the difference. I need to live in a city with a high number or density of $100,000+ households. (I would rather not adjust this for the cost of living across various cities, because it’s a ballpark figure anyway).
The $100,000+ income bracket is also a good measure of my market household for one-on-one tutoring. Most of them are high-school families. This market is much more localized; most of these clients don’t bother driving more than about four miles to my office. To maximize on this market, it’s best to find a neighborhood within a city that has a high market household density. It’s not very important to have super-rich clients. $500,000 households don’t need five times as much tutoring as $100,000 households. It’s the density of “rich enough” households that matters.
Third, I teach group “test prep” classes to college graduates applying to graduate or professional school. In this market, my clients tend to be low-to-mid income. My classes cost about half as much as the big agencies’ (like Kaplan), so I draw the bargain-hunting crowd. That works for me, because I group them together and earn a good hourly rate. Group-class students are less localized than high-school students. They sometimes drive up to 25 miles to get here, which is practical on the weekends. Living near a college would help if I could really tap into it, but that’s hard to do. Most of my students are already done with college. I’ll say my ideal environment for group classes is a metropolitan area with a high density of $50 – 100K households 3They almost always live with other earners, so this really is “low-to-mid” for 2 or 3 incomes combined. , with nearby colleges being a nice bonus.
It’s probably not possible to find a neighborhood that is optimal for all three of these markets, but I should be able to identify strong combinations. For example, areas with uniform distributions of low-, middle-, and high-income households offer some of all these markets, while also offering low-rent housing. If I had to sacrifice one of these markets for the others to grow, I would give up the one with the lowest hourly rate — high-school tutoring.
Competition
Growing your business is not just about finding a bigger market. You also want a big market share. That depends on the number and size of competing businesses. It’s a major factor that I think many entrepreneurs overlook. A friend of mine is one of the most successful immigration lawyers in Phoenix, AZ. She expanded to LA and counted on an easy-breezy doubling of her fortune. What she hadn’t counted on was the dozens of competing immigration lawyers near her LA office. Dozens — not in her neighborhood but in her freaking building. It was a market she was not prepared for. That office was closed within a few years.
My friend’s example shows that competition might not be proportional to city size. In line with that, the large national test-prep chains like Kaplan can’t be in every city. They focus on the very largest college communities in the very largest cities. I currently live between UCLA and USC, but I hardly ever get students from either school. Blueprint and Manhattan Prep occupy their campuses like invading armies. Maybe a school like Cal State Northridge or the University of Minnesota would be slightly less under their domination.
Toward a metric
If I can capture the most important factors, I can construct a sort of “earnings metric” for each city or neighborhood. From the considerations above, those factors would have to include:
A = Number of $100,000+ households within a 25-mile radius
B = Number of $100,000+ households within a 4-mile radius
C = Number of $50,000 – 100,000 households within a 25-mile radius
D = Number of competing patent lawyers within a 25-mile radius
E = Number of competing high-school tutors within a 4-mile radius
F = Number of competing test-prep centers within a 25-mile radius
Then my earnings metric would be something like:
M = 0.5(A/D) + 0.25(B/E) + 0.25(C/F)
When measured against the baseline neighborhood where I live now, M would be a good first guess for an earnings multiplier. That is, if M = 1 for Rancho Park and M = 2 for Austin, then I could reasonably expect to earn twice as much in Austin as in Rancho Park. To be more precise, each ratio will actually be a ratio of ratios: the new neighborhood ratio over my current ratio. But now we’re getting into formulas that are too hard to type in a simple blog post. 😛
The next phase of the analysis will be determining the baseline ratios for my current location: Who lives here, and who’s serving them in competition against me?


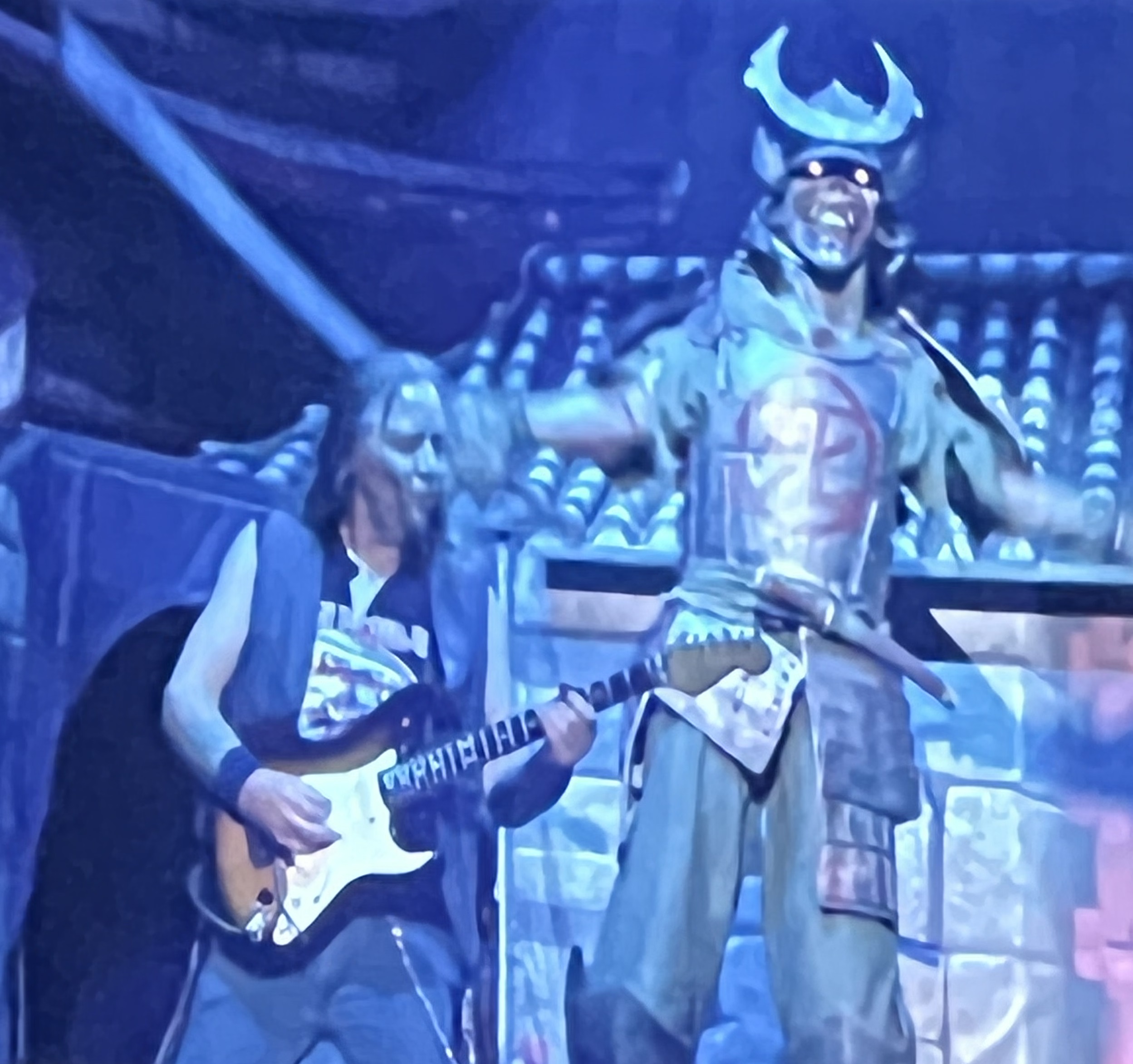
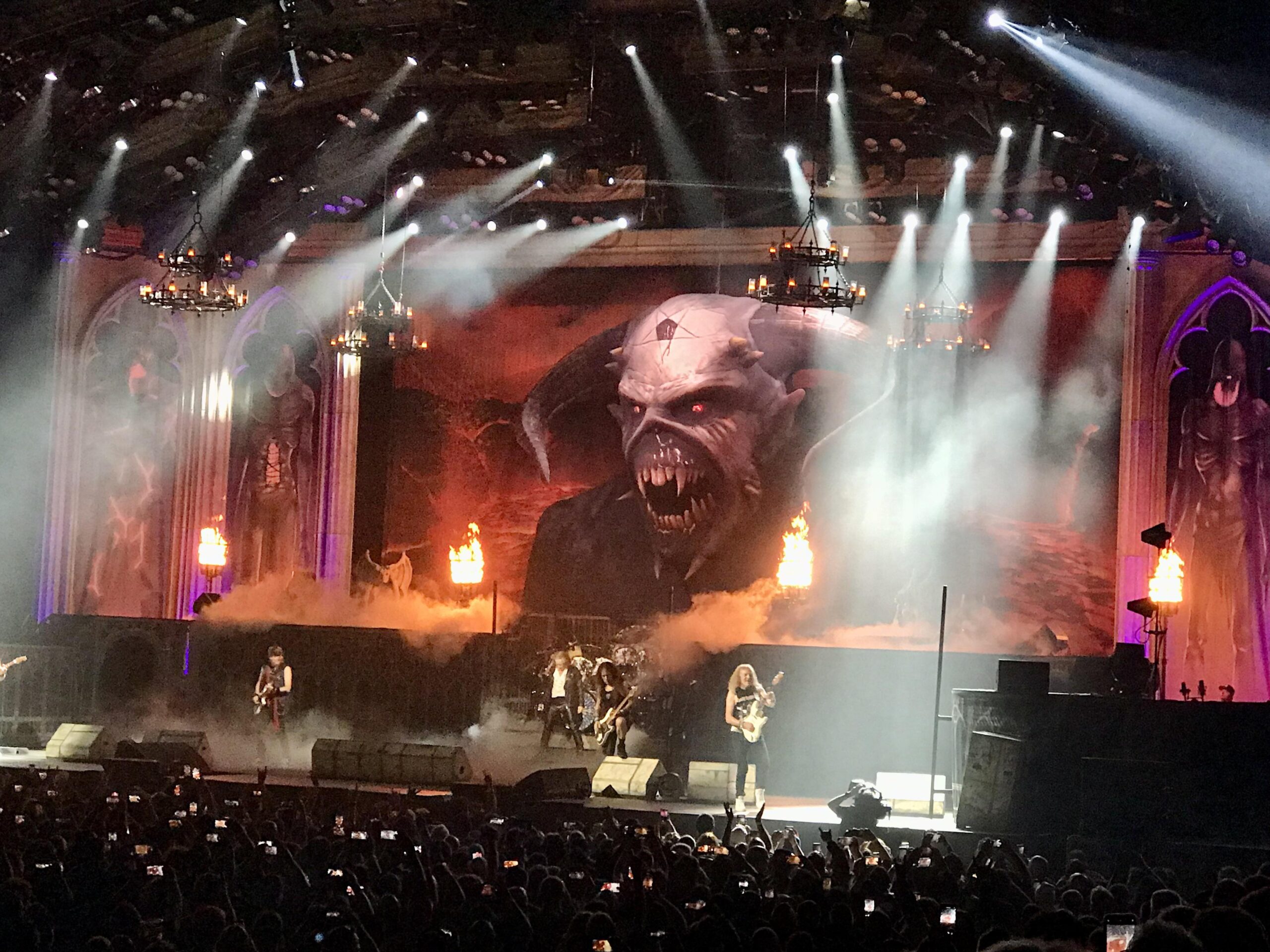
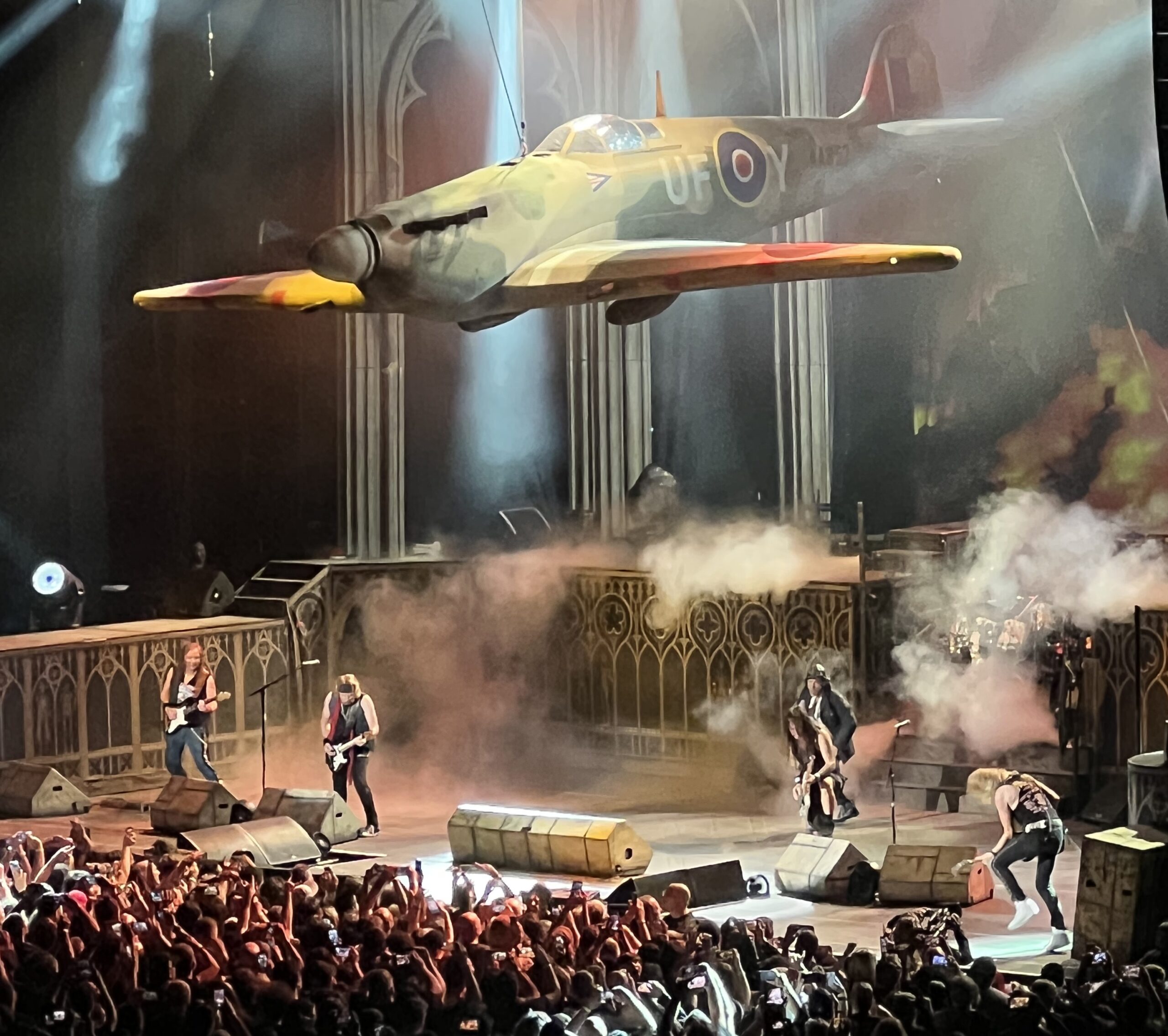

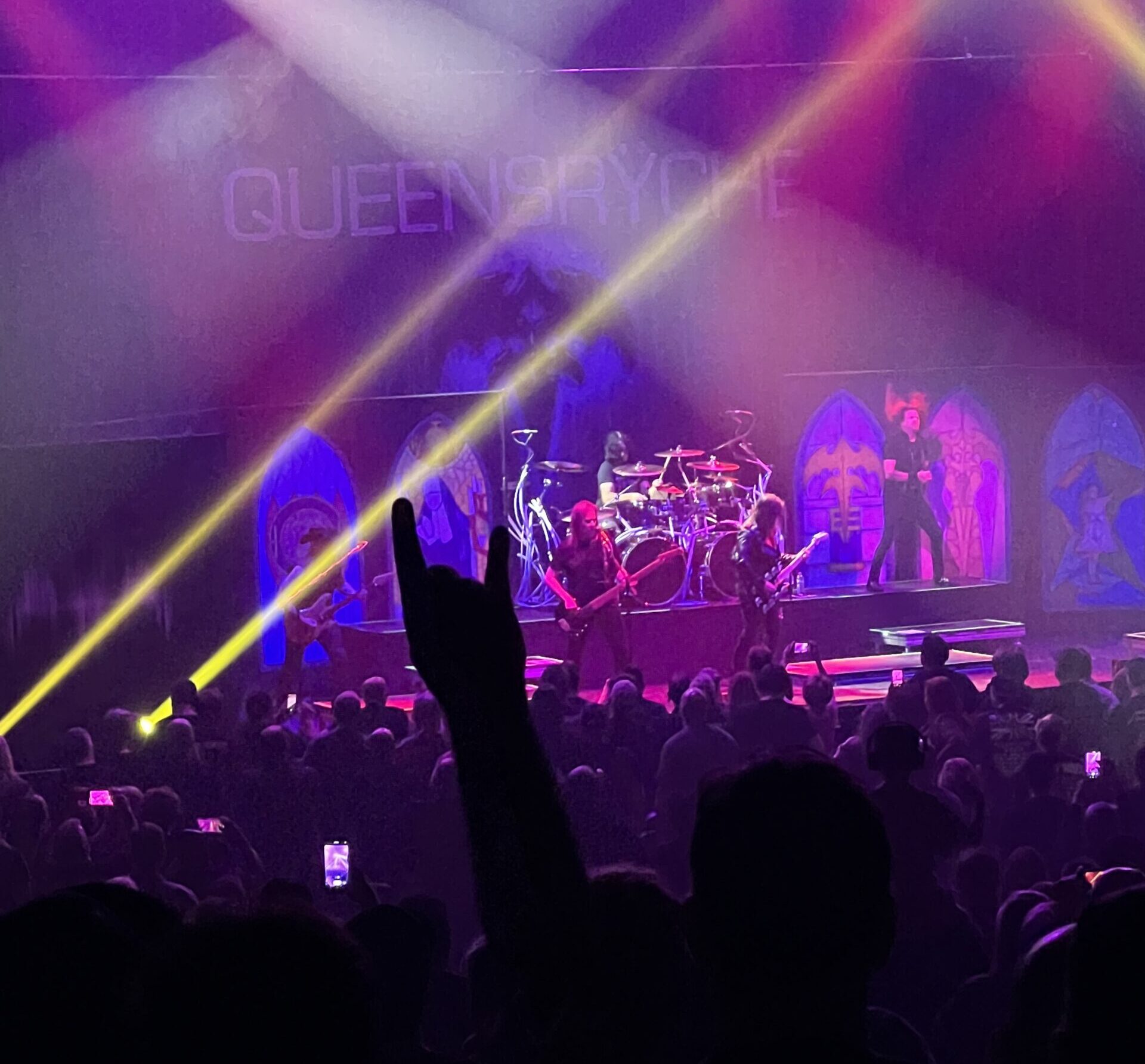

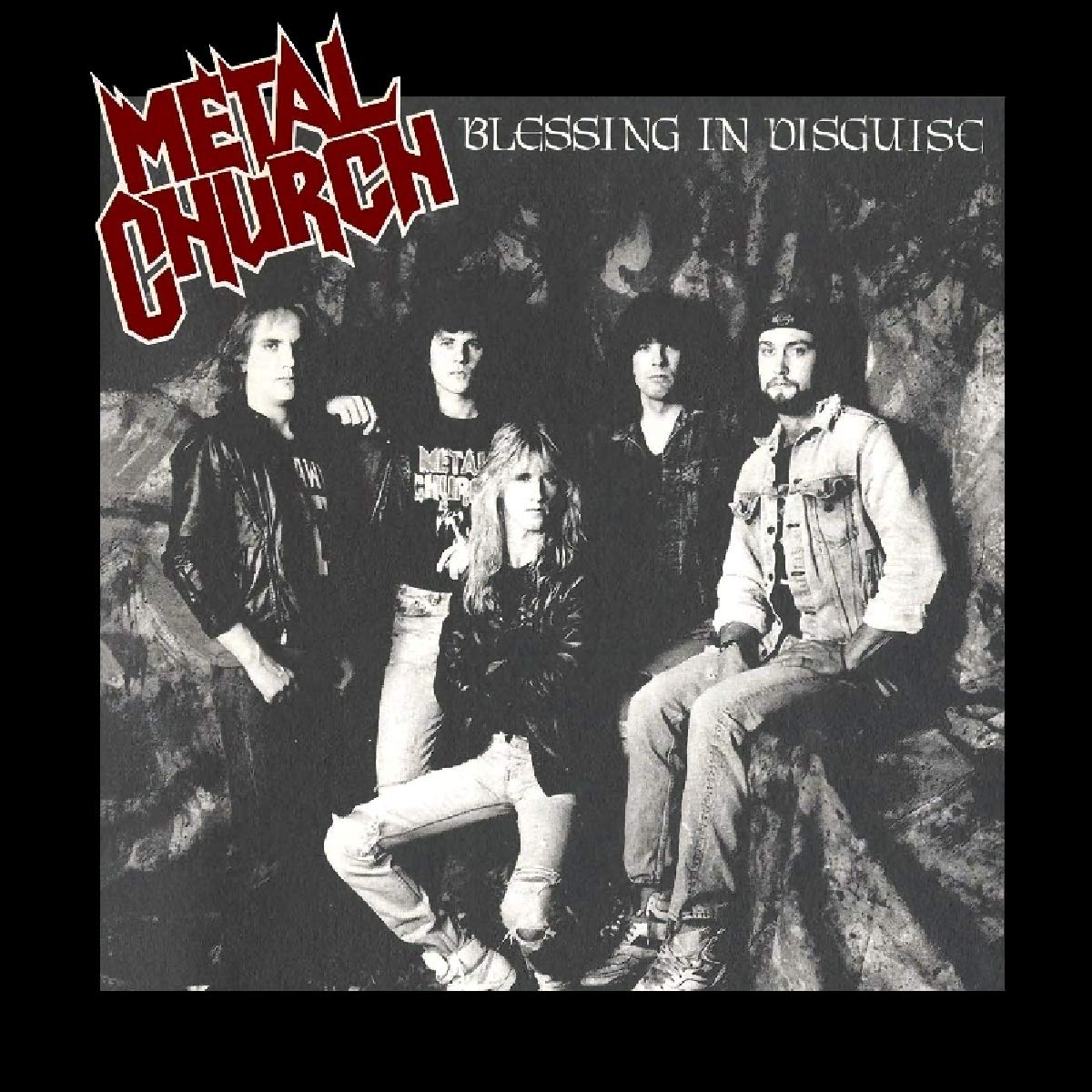




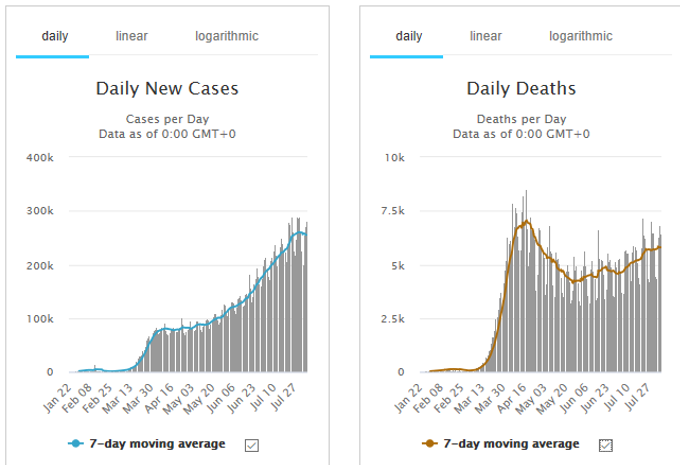
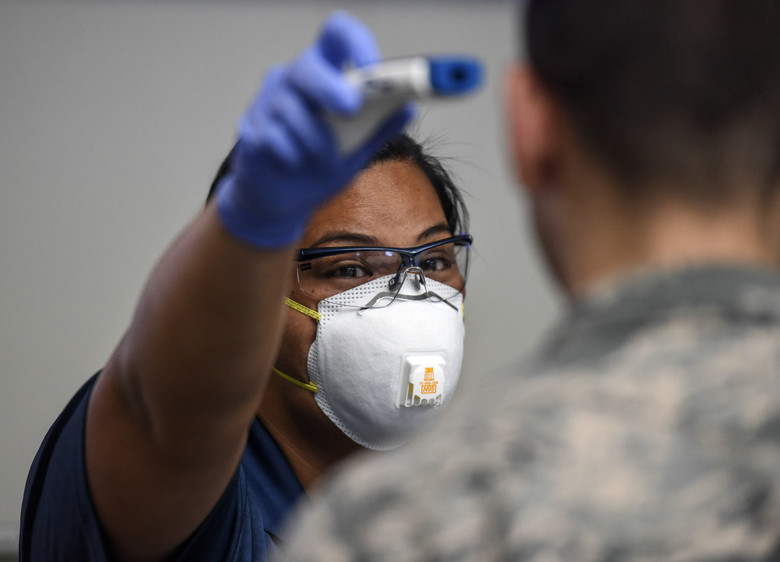

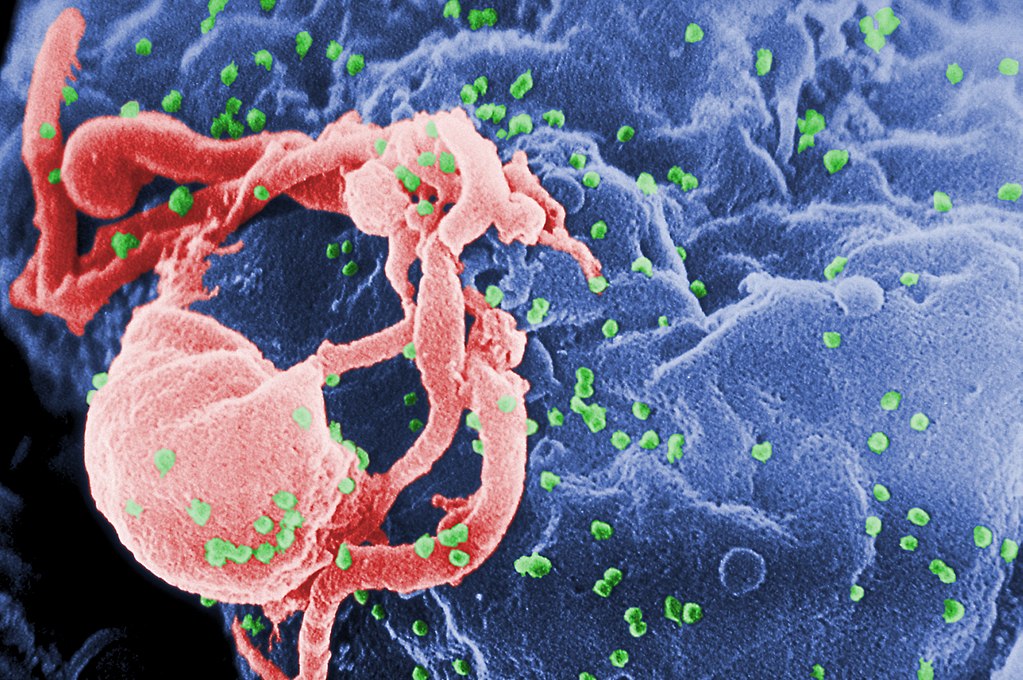
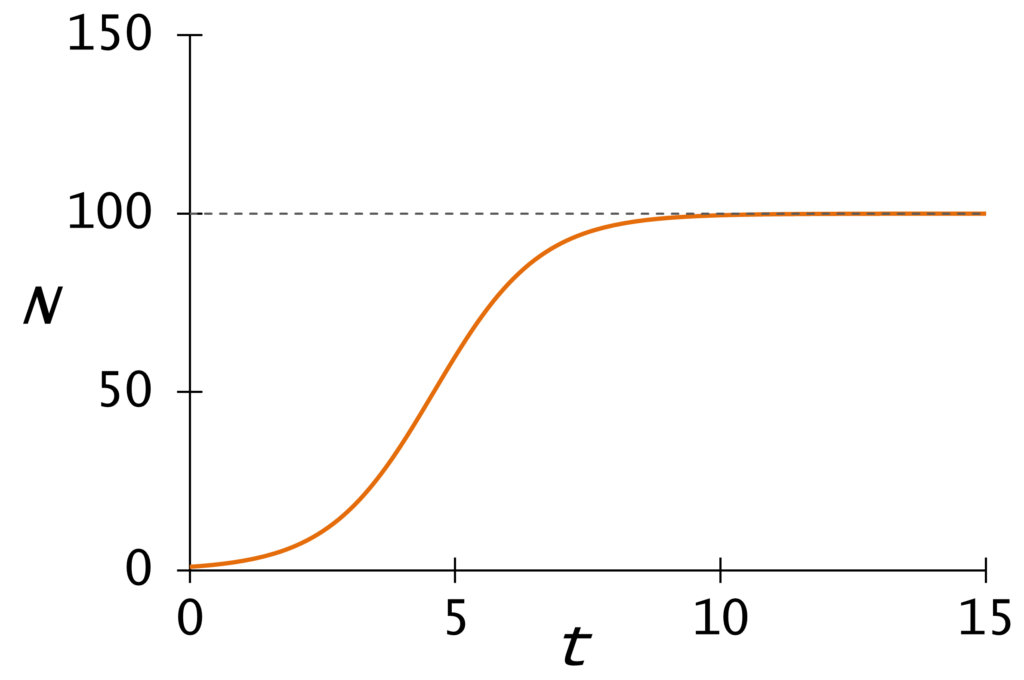
{kind=link}
{kind=link}